The nurse is caring for a one-month-old infant admitted for suspected congenital hypothyroidism. Which diagnostic test results should the nurse report to the healthcare provider?
Luteinizing hormone (LH) levels.
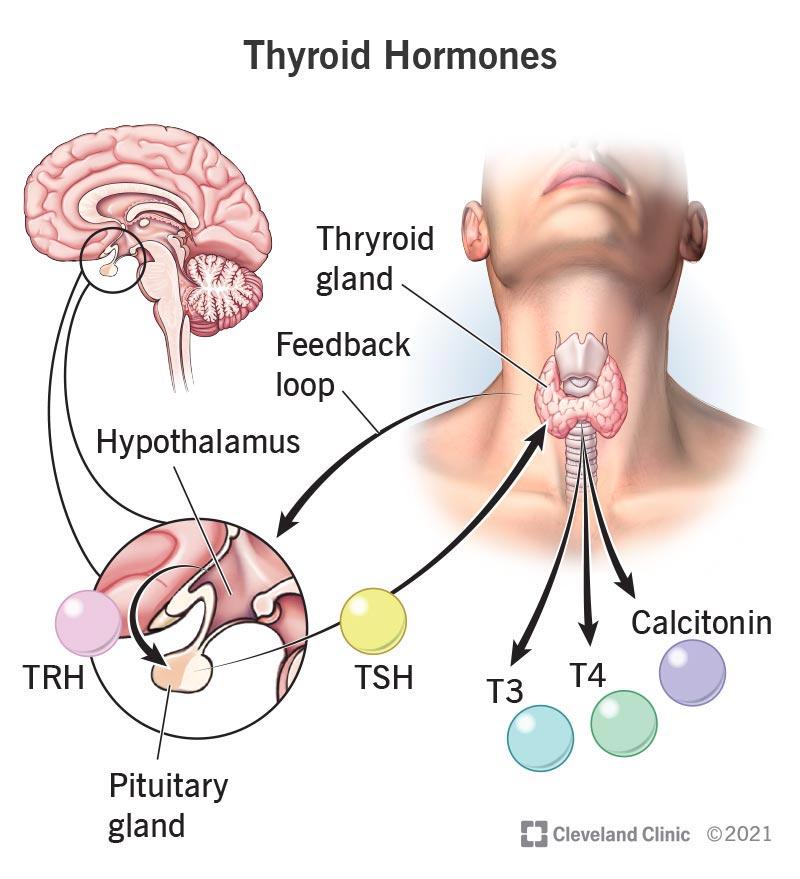
Thyroxine (T4).
Growth hormone (GH) levels.
Follicle stimulating hormone (FSH) levels.
The Correct Answer is B
Choice A reason: Luteinizing hormone (LH) levels are not relevant for the diagnosis of congenital hypothyroidism. LH is a hormone that regulates the reproductive system and is not affected by thyroid function.
Choice B reason: Thyroxine (T4) is the main hormone produced by the thyroid gland and is essential for growth and development. Low levels of T4 indicate hypothyroidism and require treatment with thyroid hormone replacement. High levels of T4 indicate hyperthyroidism and require treatment with anti-thyroid drugs.
Choice C reason: Growth hormone (GH) levels are not relevant for the diagnosis of congenital hypothyroidism. GH is a hormone that stimulates growth and metabolism and is not affected by thyroid function.
Choice D reason: Follicle stimulating hormone (FSH) levels are not relevant for the diagnosis of congenital hypothyroidism. FSH is a hormone that regulates the reproductive system and is not affected by thyroid function.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: Instilling benzocaine otic drops regularly is not a recommended practice for preventing or treating otitis media. Benzocaine is a topical anesthetic that can temporarily relieve ear pain, but it does not address the underlying cause of the infection. Moreover, benzocaine can cause allergic reactions, skin irritation, or methemoglobinemia, a condition that reduces the oxygen-carrying capacity of the blood. The nurse should instruct the caregiver to avoid using benzocaine otic drops unless prescribed by a health care provider.
Choice B reason: Avoiding any smoking inside the house is a good practice for preventing otitis media. Smoking can irritate the respiratory tract and impair the function of the cilia, the hair-like structures that help clear mucus and bacteria from the middle ear. Smoking can also increase the risk of respiratory infections, allergies, and asthma, which are associated with otitis media. The nurse should praise the caregiver for avoiding smoking and encourage them to maintain a smoke-free environment for the infant.
Choice C reason: Giving the infant the full course of antibiotics is a necessary practice for treating otitis media. Antibiotics can help eliminate the bacteria that cause the infection and reduce the inflammation and pain in the middle ear. However, antibiotics should be used only when prescribed by a health care provider, and the caregiver should follow the instructions carefully. The nurse should remind the caregiver to give the infant the exact dose of antibiotics at the right time and for the entire duration of the treatment, even if the symptoms improve.
Choice D reason: Scheduling a visit for pneumococcal vaccine is a preventive measure for otitis media. Pneumococcal vaccine can protect the infant from the most common strains of Streptococcus pneumoniae, a bacterium that causes otitis media and other serious infections. The vaccine is recommended for all children under 2 years of age, and it is given in four doses at 2, 4, 6, and 12 to 15 months of age. The nurse should verify the infant's immunization status and advise the caregiver to follow the recommended schedule for the pneumococcal vaccine.

Correct Answer is A
Explanation
Choice A reason: Rice is a gluten-free grain that is safe for people with celiac disease. Rice does not contain the protein gluten that triggers an immune reaction and damages the small intestine in people with celiac disease.
Choice B reason: Oats are generally not recommended for people with celiac disease because they are often contaminated with gluten from other grains during processing. Some people with celiac disease may also react to a protein in oats called avenin that is similar to gluten. Only certified gluten-free oats may be safe for some people with celiac disease, but they should consult their health care provider before consuming them³.
Choice C reason: Barley is a grain that contains gluten and is not safe for people with celiac disease. Barley can cause inflammation and damage to the small intestine in people with celiac disease. Barley is also used to make malt, which is a common additive in many processed foods and beverages.
Choice D reason: Rye is a grain that contains gluten and is not safe for people with celiac disease. Rye can cause the same symptoms and complications as wheat and barley in people with celiac disease. Rye is often used to make bread, crackers, and cereals.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today