
Ati nurse 142 final
Ati nurse 142 final
Total Questions : 45
Showing 10 questions Sign up for moreThe nurse is caring for two clients who both are in pain due to sickle cell anemia. One of the clients rates the pain as a 7 out of 10 (0 is no pain and 10 is the worst pain possible). This client is moving around easily and is eating well, but has asked for pain medication. Which action by the nurse is most appropriate?
Explanation
Pain is a subjective experience, and the client's report of pain should be respected and addressed promptly. If the pain medication is ordered and it has been longer than the ordered interval, the nurse should administer the medication as prescribed. In general, withholding pain medication for a client in pain is not an appropriate action.
Administering half the ordered dose of pain medication without a healthcare provider's order is also not appropriate. The nurse should follow the healthcare provider's orders for pain medication administration and titration.
It's also not appropriate to assume that the client is faking pain without adequate assessment and evidence to support such a claim. The nurse should perform a thorough pain assessment, including the location, intensity, and quality of the pain, and consider non-pharmacological interventions to help manage the pain.
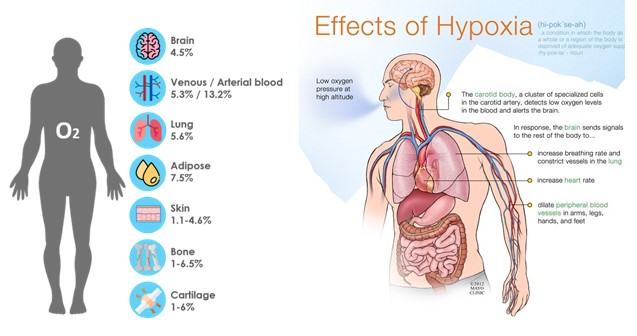
The nurse is assessing the patient's lips and notes a bluish tinge. This finding would indicate that the patient may be experiencing which problem?
Explanation
Hypoxia is a medical condition characterized by a lack of oxygen in the body's tissues, which can occur due to a variety of reasons, such as respiratory failure, cardiac arrest, or other serious medical conditions. Cyanosis occurs when the oxygen saturation level in the blood falls below 85%, which causes a bluish color to appear on the skin, especially on the lips and fingertips. Therefore, if a nurse observes cyanosis in a patient's lips, it is a significant sign of hypoxia, and the patient requires immediate medical attention.
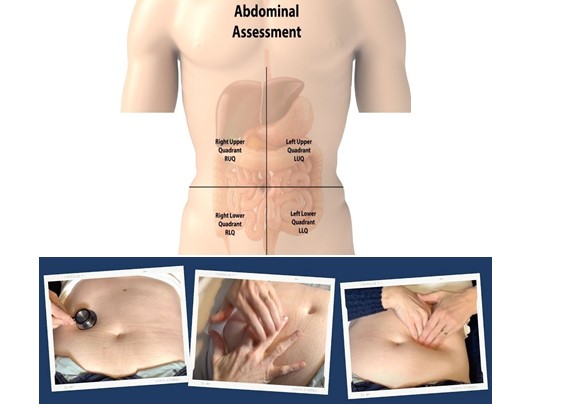
When assessing the abdomen, the nurse would expect to auscultate which sounds?
Explanation
When assessing the abdomen, the nurse would expect to auscultate bowel sounds, which are the sounds made by the movement of gas and fluid through the intestines. The normal bowel sounds are characterized as high-pitched, gurgling, and occurring at a rate of 5-30 sounds per minute.
Bruits are abnormal sounds indicating turbulent blood flow and are usually assessed in other areas of the body, such as the epigastric and renal arteries, as well as in the aorta.
Friction rubs are also abnormal sounds, but they are typically heard during auscultation of the heart and lungs.
Low-pitched sonorous sounds are not typical sounds that are expected to be heard during an abdominal assessment
The nurse is performing a nutritional assessment. Which of the following would be considered objective data?
Explanation
Objective data are measurable and observable findings that can be obtained through physical examination, laboratory tests, or other diagnostic procedures.
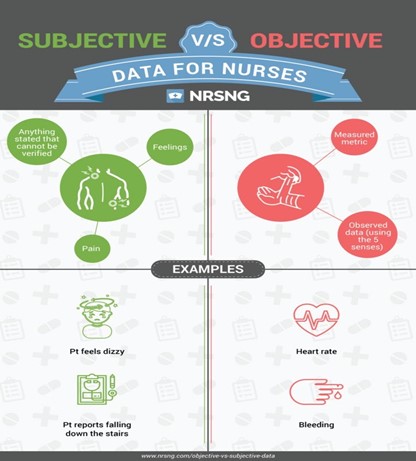
Option A is subjective data because it is information reported by the patient and may not be entirely accurate. Option Bis also subjective data because it is the patient's perception of their weight loss, which may not be an accurate reflection of actual weight loss.
Option Dis also subjective data because it relies on the patient's self-report of their alcohol intake, which may not be entirely accurate.
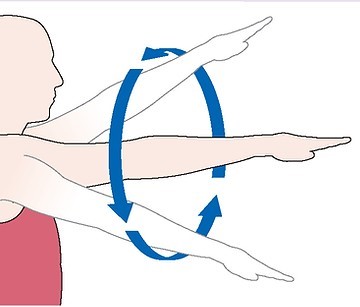
The nurse is assessing the patient's range of motion. The nurse asks the patient to circumduct his arms. When the patient asks what this means, the nurse explains:
Explanation
Circumduction is a movement that involves the circular rotation of a limb, such as an arm or leg, around a fixed point. When assessing the patient's range of motion, the nurse may ask the patient to perform circumduction of their arms to evaluate their ability to move their arms in a circular motion.
When assessing the anus, the nurse should inspect for: (Select all that apply)
Explanation
Prostate enlargement is not directly assessed through an anal examination.

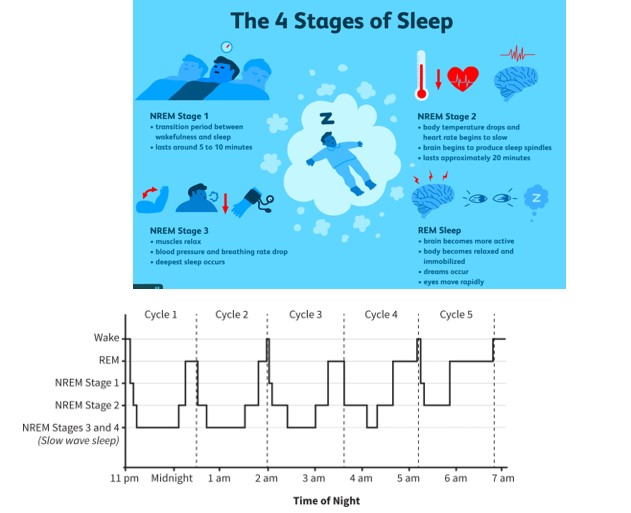
The nurse is teaching the patient about different stages of sleep. The nurse knows that REM sleep includes which one of the following?
Explanation
REM (Rapid Eye Movement) sleep is a stage of sleep that is part of the sleep cycle, which also includes non-REM (NREM) sleep. Dreaming occurs during REM sleep, and it usually composes about 20-25% of total sleep time in adults. NREM sleep, on the other hand, makes up the largest amount of total sleep time, typically about 75-80%. Both REM and NREM sleep are important for restorative sleep, but each plays a different role in physiological and cognitive functioning.
The nurse is assessing the patients sleep habits. Which of the patients responses indicate a need for the nurse to provide teaching?
Explanation
Napping during the day can interfere with a person's ability to sleep at night, especially if it is done for long periods or close to bedtime. The nurse can provide education on proper sleep hygiene and recommend ways to establish a consistent sleep schedule that promotes restful sleep, such as avoiding caffeine and alcohol, practicing relaxation techniques, and limiting exposure to electronic devices before bedtime.
In the SBAR reporting system, which of the following would be an example of a recommendation?
Explanation
The SBAR (Situation, Background, Assessment, Recommendation) system is a standardized way of communicating critical information between healthcare professionals, particularly during patient handoffs or when escalating a concern.
The recommendation component is where the healthcare professional providing the report suggests a course of action or plan for the patient based on the situation, background, and assessment. For example, a recommendation might be, "I recommend increasing Mr. Smith's pain medication to manage his discomfort," or "I recommend a consult with the nutritionist to address Mrs. Brown's malnutrition."

Of the options provided, (a) provides the situation, (c) provides the assessment, and (d) provides a specific finding from the assessment. Option (b) is a specific recommendation or plan.
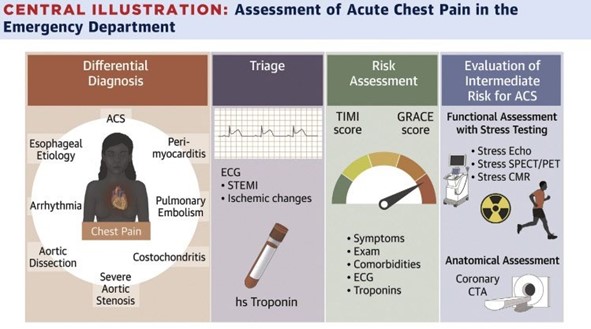
A patient is admitted to the floor with a diagnosis of chest pain. Which of the following would be a priority for the assessment?
Explanation
When a patient is admitted with a complaint of chest pain, the priority assessment would be to determine whether the patient is experiencing an acute cardiac event, such as a heart attack. This would involve a comprehensive assessment that includes obtaining the patient's medical history, vital signs (blood pressure, heart rate, respiratory rate, oxygen saturation), performing a physical exam, and obtaining an electrocardiogram (ECG).
Other important factors to assess include the location and nature of the pain, any associated symptoms (such as shortness of breath or diaphoresis), the patient's current medications and medical history (including any history of heart disease or risk factors), and any recent procedures or interventions that may have led to the current presentation.
Prompt assessment and intervention are crucial in managing a patient with chest pain, as timely treatment can help to minimize damage to the heart muscle and prevent further complications. Therefore, any signs of an acute cardiac event should be immediately reported to the healthcare provider in charge, and appropriate interventions should be initiated promptly.
You just viewed 10 questions out of the 45 questions on the Ati nurse 142 final Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

