At the beginning of your shift, you start your rounds on your patients. Upon entering this patient’s room, you observe that the cardiac monitor shows sinus tachycardia, is apneic and no pulses are palpable by the nurse.
What is the first action that the nurse should take?
Administer the prescribed Beta-Blocker
Prepare for Cardioversion per hospital protocol.
Give 100% oxygen per non-rebreather mask.
Start CPR
The Correct Answer is D
The absence of palpable pulses suggests a lack of effective cardiac output, and the patient is in cardiac arrest. In this situation, immediate initiation of cardiopulmonary resuscitation (CPR) is crucial to maintain circulation and provide oxygenation to vital organs.
CPR consists of chest compressions and rescue breaths to circulate oxygenated blood to the brain and other vital organs. It is the primary intervention in cardiac arrest to provide temporary life support until advanced cardiac life support (ACLS) measures, such as defibrillation or medication administration, can be initiated.
A. Administering the prescribed Beta-Blocker in (option A) is incorrect because Administering a beta-blocker is not the initial action in a patient who is in cardiac arrest and requires immediate resuscitation.
B. Prepare for Cardioversion per hospital protocol (option B) is incorrect because Cardioversion, which is the delivery of an electric shock to the heart, may be considered in certain situations like unstable ventricular tachycardia or certain supraventricular tachycardias. However, in the given scenario, the patient is unresponsive and has no pulses, indicating cardiac arrest where CPR takes precedence over cardioversion.
C. Give 100% oxygen per non-rebreather mask in (option C) is incorrect because: While oxygenation is important, it should not delay or replace the initiation of CPR, which is the immediate priority in a patient without palpable pulses.
Therefore, the first action that the nurse should take in this scenario is to start CPR.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
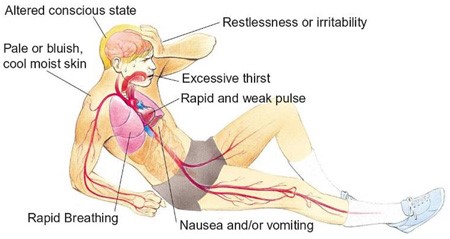
Hypovolemic shock is a life-threatening condition resulting from severe blood or fluid loss. The patient in this scenario exhibits signs of hypovolemic shock, such as low blood pressure, tachycardia, cool and clammy skin, and decreased urine output.
When assessing the prescription options, the nurse should consider the appropriateness of each intervention for hypovolemic shock. Plasmanate is a type of plasma protein fraction that is used for volume expansion in certain situations. However, in hypovolemic shock, the primary intervention is to restore intravascular volume promptly. Plasmanate alone may not be sufficient for rapid-volume resuscitation.
In hypovolemic shock, the initial management typically involves the administration of crystalloid solutions, such as Lactated Ringers or Normal Saline, to restore intravascular volume. Therefore, the prescription of Plasmanate as the primary intervention raises concerns and should be questioned by the nurse.
A. Dopamine (Intropin) 12 mcg/min in (option A) is incorrect because: Dopamine is a vasopressor medication used to increase blood pressure and cardiac output. It is a suitable option for hypovolemic shock to support blood pressure and tissue perfusion.
B. Dobutamine (Dobutrex) 5 mcg/kg/min in (option B) is incorrect because: Dobutamine is an inotropic medication that helps improve cardiac contractility and cardiac output. It can be beneficial in cases of hypovolemic shock with signs of poor cardiac function.
D. Bumetanide (Bumex) 1 mg IV in (option D) is incorrect because: Bumetanide is a loop diuretic used to promote diuresis. However, in the context of hypovolemic shock, diuretics are generally not the first-line treatment as they can further reduce intravascular volume and worsen the patient's condition.
It is essential for the nurse to consult with the healthcare provider regarding the prescription order of Plasmanate and consider alternative interventions for rapid volume resuscitation in hypovolemic shock.
Correct Answer is ["A","B","C"]
Explanation
These conditions can lead to fluid loss, either through increased gastrointestinal output (diarrhea, vomiting, lower GI bleeding) or accumulation of air in the pleural space (tension pneumothorax), resulting in a decrease in blood volume and subsequent hypovolemic shock.
E. Diabetes insipidus in (option E) is incorrect because it is not directly associated with hypovolemic shock. Diabetes insipidus is a condition characterized by excessive thirst and the production of large volumes of dilute urine due to insufficient production or response to antidiuretic hormone (ADH). While diabetes insipidus can lead to dehydration and potential hypovolemia, it is not a direct cause of hypovolemic shock.
F. Valvular stenosis in (option F) is incorrect because it is a condition characterized by the narrowing or obstruction of one or more heart valves. While it can cause problems with cardiac output and circulation, it is not specifically related to hypovolemic shock, which is caused by a decrease in blood volume.
Therefore, the conditions that can cause hypovolemic shock include diarrhea, vomiting, lower GI bleeding, and tension pneumothorax.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today