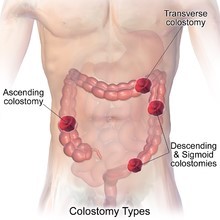
A nurse is reinforcing teaching with another nurse about how to change an ostomy appliance for a client who has a sigmoid colostomy.
Which of the following instructions should the nurse include in the teaching?
Create an opening on the skin barrier that is 1.27 cm (0.5 in) larger than the client's stoma
Use a moisturizing soap to clean the skin around the client's stoma
Empty the client's ostomy pouch before removing the skin barrier
Change the client's ostomy appliance 1 hr after breakfast
Correct Answer : C
A. Create an opening on the skin barrier that is 1.27 cm (0.5 in) larger than the client's stoma. The opening on the skin barrier should be cut to fit closely around the stoma, approximately 0.3-0.6 cm (1/8 to 1/4 inch) larger than the stoma size. A larger opening (like 0.5 inches) could expose too much surrounding skin, increasing the risk of skin irritation from contact with the stoma's effluent.
B. Use a moisturizing soap to clean the skin around the client's stoma. Moisturizing soaps should be avoided because they can leave a residue on the skin, which may interfere with the adhesion of the ostomy appliance. The skin around the stoma should be cleaned with mild soap and water, or water alone, and then dried thoroughly before applying the new appliance.
C. Empty the client's ostomy pouch before removing the skin barrier. Emptying the ostomy pouch before removing the skin barrier is a practical step to reduce spillage of stool during the appliance change, making the process cleaner and easier to manage. It also minimizes the risk of contamination of the surrounding area or wound.
D. Change the client's ostomy appliance 1 hour after breakfast. Ostomy appliances are best changed when the bowel is least active, which is usually before a meal or several hours after eating. Changing the appliance shortly after a meal, such as 1 hour after breakfast, may result in more stoma output, making it harder to manage the appliance change.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Explanation
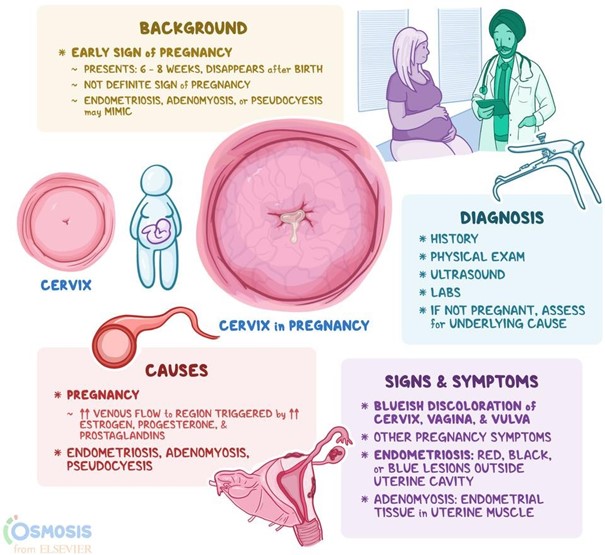
A. Chadwick’s sign
Chadwick's sign is a characteristic change that occurs during pregnancy, specifically in the cervix, vagina, and vulva. It is characterized by a bluish or purplish discoloration of these areas.
Chloasma in (option B) is incorrect because it is a condition characterized by the development of dark patches on the skin, commonly referred to as "mask of pregnancy." Chloasma typically affects the face, particularly the cheeks, forehead, and upper lip. It is not associated with a change in colour in the vaginal or vulvar area.
Hegar's sign in (option C) is incorrect because it is a softening of the lower uterine segment that can be felt during a pelvic examination. It is not related to the colour changes in the vaginal or vulvar area.
Ballottement in (option D) is incorrect because it is a palpation technique used during a prenatal examination to assess the position of the foetus. It involves the examiner gently pushing against the uterus and feeling a rebound or "floating" movement of the foetus. It does not involve changes in the colour of the vaginal or vulvar area.
Correct Answer is D
Explanation
Correct answer: D
a.Artificial flowers are generally considered safer than fresh flowers because they do not harbor water, which can be a source of bacterial growth. However, they can collect dust, which might carry pathogens, though this is typically a lesser concern compared to fresh flowers.
b. Being assigned to a room with negative airflow is actually beneficial for a client with an immunocompromised condition, as it helps prevent the spread of airborne pathogens.
c.Hard boiled eggs do not inherently increase the risk of infection. However, it is important to ensure that all food items are properly prepared, handled, and stored to minimize the risk of foodborne illnesses.
d. Fresh fruit can harbor bacteria and other pathogens on their surfaces, which can pose a significant risk to a neutropenic patient. Even with thorough washing, there is a higher risk compared to cooked or pasteurized foods.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today