A nurse is assisting with the admission of a child who has measles. Which of the following isolation precautions should the nurse initiate?
Contact
Airborne
Protective environment
Droplet
The Correct Answer is B
Choice A: Contact isolation is not appropriate for a child who has measles, which is a highly contagious viral infection that causes fever, rash, cough, runny nose, and red eyes. Contact isolation is used for patients who have infections that can be spread by direct or indirect contact with the patient or their environment, such as wound infections, scabies, or Clostridioides difficile. Contact isolation requires wearing gloves and gowns and using dedicated equipment.
Choice B: Airborne isolation is appropriate for a child who has measles, as it is used for patients who have infections that can be spread by small droplets that can remain suspended in the air and travel over long distances, such as tuberculosis, chickenpox, or measles. Airborne isolation requires wearing a respirator mask and placing the patient in a negative pressure room with the door closed.
Choice C: Protective environment isolation is not appropriate for a child who has measles, as it is used for patients who have compromised immune systems and are at high risk of acquiring infections from others, such as transplant recipients, cancer patients, or patients receiving immunosuppressive therapy. Protective environment isolation requires wearing gloves, gowns, masks, and eye protection and placing the patient in a positive pressure room with high-efficiency particulate air (HEPA) filters.
Choice D: Droplet isolation is not appropriate for a child who has measles, as it is used for patients who have infections that can be spread by large droplets that can travel up to 6 feet from the source, such as influenza, pertussis, or meningitis. Droplet isolation requires wearing a surgical mask and eye protection and placing the patient in a private room or cohorting with other patients with the same infection.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A: This response is appropriate, as it informs the parent that reporting suspected child abuse is a legal and ethical obligation for nurses, regardless of their personal opinions or feelings. This response also shows respect and honesty by acknowledging the parent's concern and explaining the reason for the nurse's action.
Choice B: This response is not appropriate, as it deflects responsibility and avoids answering the parent's question. This response also shows disrespect and dishonesty by implying that the provider is more qualified or authorized to explain the situation than the nurse.
Choice C: This response is not appropriate, as it denies information and creates confusion for the parent. This response also shows indifference and avoidance by suggesting that the nurse does not want to deal with the issue or communicate with the parent.
Choice D: This response is not appropriate, as it shifts blame and undermines trust between the nurse and the parent. This response also shows defensiveness and insecurity by implying that the nurse did not make the decision or take accountability for their action.
Correct Answer is C
Explanation
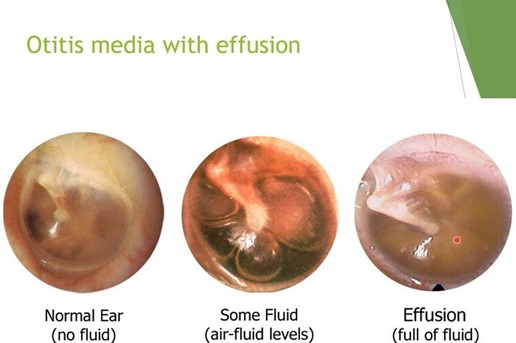
Choice A: A popping sensation when swallowing is not a sign of a tympanic membrane rupture, as it is a normal phenomenon that occurs when the eustachian tube opens and closes to equalize the pressure between the middle ear and the atmosphere. A popping sensation when swallowing may be associated with otitis media with effusion, which is a condition that causes fluid accumulation behind the eardrum, but it does not indicate a rupture.
Choice B: Green-blue discharge could be indicative of infection but is not as directly related to the rupture event as the sudden pain relief is.
Choice C: The correct answer is sudden relief of pain. This is because the rupture of the tympanic membrane releases the pressure and fluid that has built up in the middle ear, leading to an immediate decrease in pain.
Choice D: An increased temperature is not a sign of a tympanic membrane rupture, as it is a nonspecific symptom that may indicate various conditions, such as inflammation, infection, or fever. An increased temperature may be associated with otitis media with effusion, which is a condition that causes fluid accumulation behind the eardrum, but it does not indicate a rupture.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today