A nurse is caring for a child who has influenza. The nurse should identify which of the following statements by the parent indicates the child has an increased risk for Reye syndrome.
"I give my child ibuprofen when his muscles are aching."
"I am encouraging my child to drink grapefruit juice."
"I am leaving a humidifier on in my child's room when he naps."
"I give my child aspirin to reduce his fever."
The Correct Answer is D
Choice A: Ibuprofen is a nonsteroidal anti-inflammatory drug (NSAID) that can be used to relieve pain and inflammation in children with influenza. Ibuprofen does not increase the risk of Reye syndrome, which is a rare but serious condition that affects the brain and liver.
Choice B: Grapefruit juice is a citrus fruit that can provide vitamin C and hydration for children with influenza. Grapefruit juice does not increase the risk of Reye syndrome, but it can interact with some medications and affect their absorption or metabolism.
Choice C: A humidifier is a device that adds moisture to the air and can help ease congestion and coughing in children with influenza. A humidifier does not increase the risk of Reye syndrome, but it should be cleaned regularly to prevent bacterial growth and infection.
Choice D: Aspirin is a salicylate that can be used to reduce fever and inflammation in children with influenza. However, aspirin can increase the risk of Reye syndrome, especially in children who have viral infections. Reye syndrome can cause swelling in the brain, liver damage, and even death. Therefore, aspirin should be avoided in children under 19 years old who have influenza or other viral illnesses.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: This choice is incorrect because mumps is not the common name for pertussis. Mumps is a viral infection that causes inflammation of the salivary glands, especially the parotid glands. It may cause symptoms such as fever, headache, and swelling of the cheeks or jaw. It can be prevented by vaccination with the measles-mumps-rubella (MMR) vaccine.
Choice B reason: This choice is correct because whooping cough is the common name for pertussis. Pertussis is a bacterial infection that causes severe coughing spells, which may be followed by a high-pitched whoop sound or vomiting. It may cause complications such as pneumonia, seizures, or brain damage, especially in infants and young children. It can be prevented by vaccination with the diphtheria-tetanus-pertussis (DTaP) vaccine.
Choice C reason: This choice is incorrect because the fifth disease is not the common name for pertussis. The fifth disease is a viral infection that causes a rash on the face, trunk, and limbs, which may resemble a slapped cheek appearance. It may cause mild symptoms such as fever, runny nose, or joint pain. It usually affects children and is self-limiting.
Choice D reason: This choice is incorrect because chickenpox is not the common name for pertussis. Chickenpox is a viral infection that causes an itchy rash with fluid-filled blisters all over the body. It may cause symptoms such as fever, headache, or loss of appetite. It can be prevented by vaccination with the varicella-zoster (VZV) vaccine.
Correct Answer is C
Explanation
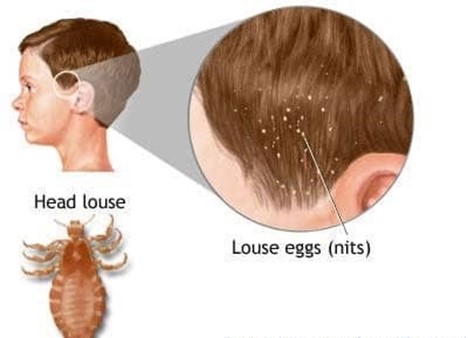
Choice A: Toys that can't be dry cleaned or washed do not need to be thrown out, as they can be treated by sealing them in plastic bags for two weeks or placing them in a freezer for two days. This will kill any lice or nits that may have been transferred from the child's head.
Choice B: Nits will not always be present, as they can be removed by using a fine-toothed comb or applying products that loosen their attachment to the hair shafts. Nits are the eggs of lice that are glued to the hair near the scalp. Nits can hatch into nymphs within seven to ten days and mature into adult lice within another seven to ten days.
Choice C: All recently used clothing, bedding, and towels must be washed in hot water, as this will kill any lice or nits that may have been transferred from the child's head. Hot water means at least 54°C/130°F for at least ten minutes. The items should also be dried in high heat for at least twenty minutes.
Choice D: Treating all the family members is not necessary, as only those who have evidence of lice or nits should be treated with medicated shampoos or lotions that kill lice and prevent re-infestation. Treating all the family members may cause unnecessary exposure to chemicals or resistance to treatment.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today