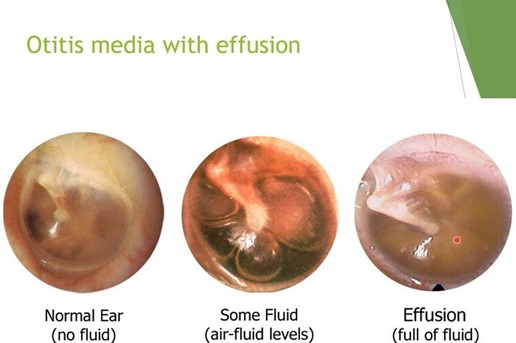
A nurse is caring for a child who has otitis media with effusion. The nurse should identify which of the following manifestations indicates a tympanic membrane rupture.
Popping sensation when swallowing
Green-blue discharge in the ear canal
Sudden pain relief
Increased temperature
The Correct Answer is C
Choice A: A popping sensation when swallowing is not a sign of a tympanic membrane rupture, as it is a normal phenomenon that occurs when the eustachian tube opens and closes to equalize the pressure between the middle ear and the atmosphere. A popping sensation when swallowing may be associated with otitis media with effusion, which is a condition that causes fluid accumulation behind the eardrum, but it does not indicate a rupture.
Choice B: Green-blue discharge could be indicative of infection but is not as directly related to the rupture event as the sudden pain relief is.
Choice C: The correct answer is sudden relief of pain. This is because the rupture of the tympanic membrane releases the pressure and fluid that has built up in the middle ear, leading to an immediate decrease in pain.
Choice D: An increased temperature is not a sign of a tympanic membrane rupture, as it is a nonspecific symptom that may indicate various conditions, such as inflammation, infection, or fever. An increased temperature may be associated with otitis media with effusion, which is a condition that causes fluid accumulation behind the eardrum, but it does not indicate a rupture.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: This choice is incorrect because tying colorful latex balloons to the side of
the crib may pose a risk of choking or suffocation for the infant who is in a cast for DDH. Latex balloons are made of rubber that can break easily and form small pieces that can block the airway or lungs if swallowed or inhaled by
the infant. Therefore, avoiding latex products such as balloons, gloves, or bandages is important to prevent accidents or injuries.
Choice B reason: This choice is incorrect because following the doctor's instructions regarding activities and treatment plans is not a specific strategy to promote the infant's growth and development. Following
the doctor's instructions regarding activities and treatment plans is a general responsibility of the nurse that applies to any client who has any condition or procedure. It may help to ensure the safety and effectiveness of the care, but it does not address the developmental needs of the infant who is in a cast for DDH.
Choice C reason: This choice is correct because providing a small electronic toy is a specific strategy to promote
the infant's growth and development. Providing a small electronic toy can help stimulate the infant's senses, cognition, and motor skills by offering visual, auditory, or tactile feedback. It may also help to reduce boredom, frustration, or depression by providing entertainment, diversion, or comfort. Therefore, providing a small electronic toy can help to enhance the developmental outcomes of the infant who is in a cast for DDH.
Choice D reason: This choice is incorrect because changing the infant's diaper as soon as soiling occurs is not a specific strategy to promote the infant's growth and development. Changing the infant's diaper as soon as soiling occurs is a general hygiene measure that applies to any infant who wears a diaper. It may help to prevent skin irritation, infection, or odor by keeping the diaper area clean and dry, but it does not address the developmental needs of the infant who is in a cast for DDH.
Correct Answer is D
Explanation
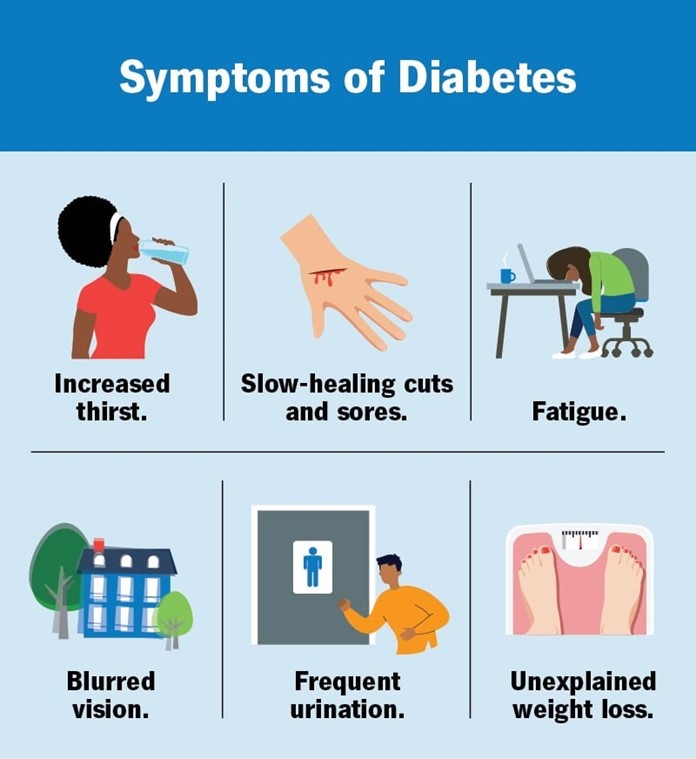
Choice A: Nausea and vomiting are not common signs of hypoglycemia, which is a low blood glucose level. Nausea and vomiting are more likely to occur with hyperglycemia, which is a high blood glucose level, or with diabetic ketoacidosis, which is a life-threatening complication of diabetes.
Choice B: Sweating is not a common sign of hyperglycemia, but rather a sign of hypoglycemia. Sweating occurs as a result of the activation of the sympathetic nervous system, which tries to raise the blood glucose level by releasing adrenaline and other hormones.
Choice C: The onset of low blood glucose usually occurs quickly, not slowly. Low blood glucose can be caused by taking too much insulin, skipping meals, exercising too much, or drinking alcohol. Low blood glucose can lead to confusion, seizures, coma, or death if not treated promptly.
Choice D: Feeling shaky is a common sign of hypoglycemia, as the body tries to cope with the lack of glucose as an energy source. Feeling shaky can also be accompanied by other signs such as hunger, nervousness, dizziness, or weakness.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today