What are the causes of a pressure ulcer? (Select all that apply.)
Ischemia
Immobility
Poor nutrition
Moisture
Adequate perfusion
Correct Answer : A,B,C,D
Choice A reason: Ischemia is a cause of a pressure ulcer, because it means reduced blood flow to the tissues, which can lead to tissue hypoxia, necrosis, and ulceration. Ischemia can result from factors such as compression, friction, shear, or vascular disease.
Choice B reason: Immobility is a cause of a pressure ulcer, because it means prolonged pressure on the bony prominences, which can impair blood flow and cause ischemia, tissue damage, and ulceration. Immobility can result from factors such as paralysis, injury, illness, or sedation.
Choice C reason: Poor nutrition is a cause of a pressure ulcer, because it means inadequate intake or absorption of nutrients, such as protein, calories, vitamins, and minerals, which are essential for tissue repair and wound healing. Poor nutrition can result from factors such as anorexia, malabsorption, or poverty.
Choice D reason: Moisture is a cause of a pressure ulcer, because it means excessive wetness or dampness of the skin, which can weaken the skin barrier, increase the risk of infection, and delay wound healing. Moisture can result from factors such as incontinence, perspiration, or wound drainage.
Choice E reason: Adequate perfusion is not a cause of a pressure ulcer, but rather a protective factor. Adequate perfusion means sufficient blood flow to the tissues, which can prevent ischemia, tissue damage, and ulceration. Adequate perfusion can be promoted by factors such as regular repositioning, pressure relief, and exercise.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: A bone fragment has injured the nerve supply in the area is not the best response by the nurse. This may be a possible complication of a fracture, but it does not explain the mechanism of compartment syndrome. Compartment syndrome is a condition where the pressure within a closed space (such as a muscle compartment) exceeds the perfusion pressure and causes ischemia and necrosis of the tissues. A bone fragment may damage the nerve, but it does not cause increased pressure in the compartment.
Choice B reason: An injured artery causes impaired arterial perfusion through the compartment is not the best response by the nurse. This may be a possible cause of compartment syndrome, but it is not the most common one. Compartment syndrome is more often caused by venous obstruction than arterial obstruction. An injured artery may reduce the blood flow to the compartment, but it does not cause increased pressure in the compartment.
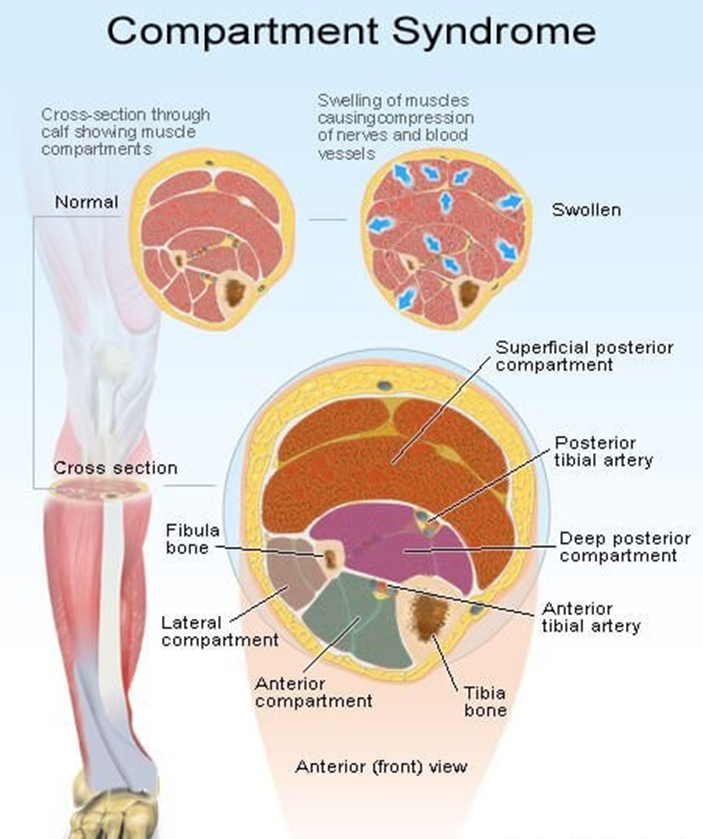
Choice C reason: Bleeding and swelling cause increased pressure in an area that cannot expand is the best response by the nurse. This is the most common cause of compartment syndrome and explains the pathophysiology of the condition. Bleeding and swelling are the result of inflammation and tissue injury that occur after a fracture. They increase the volume of fluid in the compartment, which cannot expand due to the rigid fascia that surrounds it. This leads to increased pressure in the compartment, which compresses the blood vessels, nerves, and muscles and causes ischemia and necrosis of the tissues.
Choice D reason: The fascia expands with injury, causing pressure on underlying nerves and muscles is not the best response by the nurse. This is not a correct statement, as the fascia does not expand with injury. The fascia is a tough connective tissue that encloses the muscle compartments and limits their expansion. The fascia is part of the problem, not the cause, of compartment syndrome. The fascia prevents the compartment from accommodating the increased volume of fluid and causes increased pressure in the compartment.
Correct Answer is A
Explanation
Choice A reason: This is the best intervention because it helps the nurse to understand the client's emotional, social, and practical needs and resources. A new diagnosis of HIV can be a devastating and overwhelming experience for the client, who may face stigma, discrimination, isolation, or rejection from others. The nurse should assess the client's support system, such as family, friends, or community groups, that can provide comfort, guidance, and assistance to the client. The nurse should also encourage the client to seek professional counseling, peer support, or other services as needed.
Choice B reason: This is not the best intervention because it may not respect the client's preferences, beliefs, or values. The nurse should not assume that the client wants or needs spiritual or religious support, unless the client expresses such a desire. The nurse should ask the client about their spiritual or religious beliefs and practices and provide appropriate referrals or resources as requested by the client. The nurse should also respect the client's right to privacy and confidentiality and not disclose the client's diagnosis to anyone without the client's consent.
Choice C reason: This is not the best intervention because it may not be the most urgent or appropriate topic to discuss with the client at this time. The nurse should not focus on the legal or ethical aspects of the client's diagnosis, but rather on the client's emotional and physical wellbeing. The nurse should explain the legal requirement to tell sex partners in a sensitive and respectful manner, but only after the client has accepted and understood their diagnosis and has expressed readiness to disclose their status to others. The nurse should also provide the client with information and resources on how to prevent the transmission of HIV and how to protect themselves and their partners.
Choice D reason: This is not the best intervention because it may not be the client's wish or choice. The nurse should not offer to tell the family for the client, unless the client asks for such help. The nurse should respect the client's autonomy and decisionmaking regarding whom to tell and when to tell about their diagnosis. The nurse should also support the client in preparing for the possible reactions and outcomes of disclosing their status to their family and others.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today