A wound has a bloodtinged liquid that is dripping from the surgical site. How does the nurse document this finding?
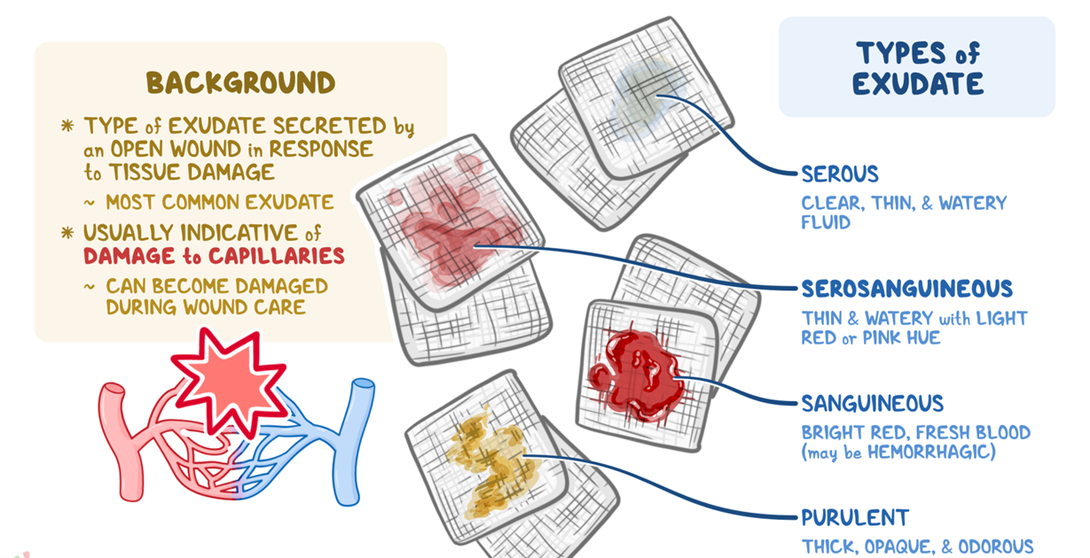
Purulent exudate
Serous exudate
Serosanguineous exudate
Sanguineous exudate
The Correct Answer is C
Choice A reason: Purulent exudate is a thick, yellowgreen, or brown pus that indicates infection. It is not bloodtinged and does not drip from the wound.
Choice B reason: Serous exudate is a clear, thin, and watery fluid that is normal in the inflammatory stage of wound healing. It does not contain blood cells and is not red in color.
Choice C reason: Serosanguineous exudate is a pink or red fluid that contains both serum and blood. It is common in the proliferative stage of wound healing and may drip from the wound due to increased capillary permeability.
Choice D reason: Sanguineous exudate is a bright or dark red fluid that consists mostly of blood. It indicates active bleeding and is usually seen in traumatic or surgical wounds. It is not diluted with serum and is more viscous than serosanguineous exudate.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: Allowing the client to sleep to build up stamina is not the priority intervention, because it does not address the psychosocial needs of the client. Sleeping is a physiological need, not a psychosocial need. Sleeping may help the client recover physically, but it does not help the client cope emotionally or socially with the isolation.
Choice B reason: Maintaining a sixfoot distance from the client is not the priority intervention, because it does not enhance the psychosocial needs of the client. Maintaining a sixfoot distance from the client is a safety measure, not a psychosocial intervention. Maintaining a sixfoot distance from the client may help prevent the transmission of infection, but it does not help the client feel less lonely or isolated.
Choice C reason: Providing a timeframe for the isolation is not the priority intervention, because it does not enhance the psychosocial needs of the client. Providing a timeframe for the isolation is an informational intervention, not a psychosocial intervention. Providing a timeframe for the isolation may help the client understand the rationale and duration of the precautions, but it does not help the client feel more engaged or supported.
Choice D reason: Providing the client with diversional activities is the priority intervention, because it enhances the psychosocial needs of the client. Providing the client with diversional activities is a psychosocial intervention, not a physiological, safety, or informational intervention. Providing the client with diversional activities may help the client feel more entertained, stimulated, and connected with others, which can reduce the negative effects of isolation.
Correct Answer is C
Explanation
Choice A reason: This is not the correct answer because opioids are a class of medications that act on the opioid receptors in the brain and spinal cord to reduce pain perception and emotional response. Opioids do not have a direct effect on tissue inflammation or bone healing, but they can cause side effects such as constipation, nausea, sedation, respiratory depression, and addiction.
Choice B reason: This is not the correct answer because anticoagulants are a class of medications that prevent or reduce the formation of blood clots by interfering with the clotting factors or platelets. Anticoagulants do not have a direct effect on tissue inflammation or bone healing, but they can increase the risk of bleeding and hematoma formation, which can impair the blood supply and oxygen delivery to the injured tissues.
Choice C reason: This is the correct answer because NSAIDs are a class of medications that inhibit the enzyme cyclooxygenase (COX), which is involved in the synthesis of prostaglandins, which are inflammatory mediators that cause pain, swelling, and fever. NSAIDs can decrease tissue inflammation and pain, but they can also delay bone healing by reducing the formation of osteoblasts, which are cells that build new bone tissue.
Choice D reason: This is not the correct answer because narcotics are another term for opioids, which are a class of medications that act on the opioid receptors in the brain and spinal cord to reduce pain perception and emotional response. Narcotics do not have a direct effect on tissue inflammation or bone healing, but they can cause side effects such as constipation, nausea, sedation, respiratory depression, and addiction.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today