The nurse is caring for a client who develops compartment syndrome from a severely fractured arm. The client asks the nurse why this can happen. What is the best response by the nurse?
A bone fragment has injured the nerve supply in the area.
An injured artery causes impaired arterial perfusion through the compartment.
Bleeding and swelling cause increased pressure in an area that cannot expand.
The fascia expands with injury, causing pressure on underlying nerves and muscles.
The Correct Answer is C
Choice A reason: A bone fragment has injured the nerve supply in the area is not the best response by the nurse. This may be a possible complication of a fracture, but it does not explain the mechanism of compartment syndrome. Compartment syndrome is a condition where the pressure within a closed space (such as a muscle compartment) exceeds the perfusion pressure and causes ischemia and necrosis of the tissues. A bone fragment may damage the nerve, but it does not cause increased pressure in the compartment.
Choice B reason: An injured artery causes impaired arterial perfusion through the compartment is not the best response by the nurse. This may be a possible cause of compartment syndrome, but it is not the most common one. Compartment syndrome is more often caused by venous obstruction than arterial obstruction. An injured artery may reduce the blood flow to the compartment, but it does not cause increased pressure in the compartment.
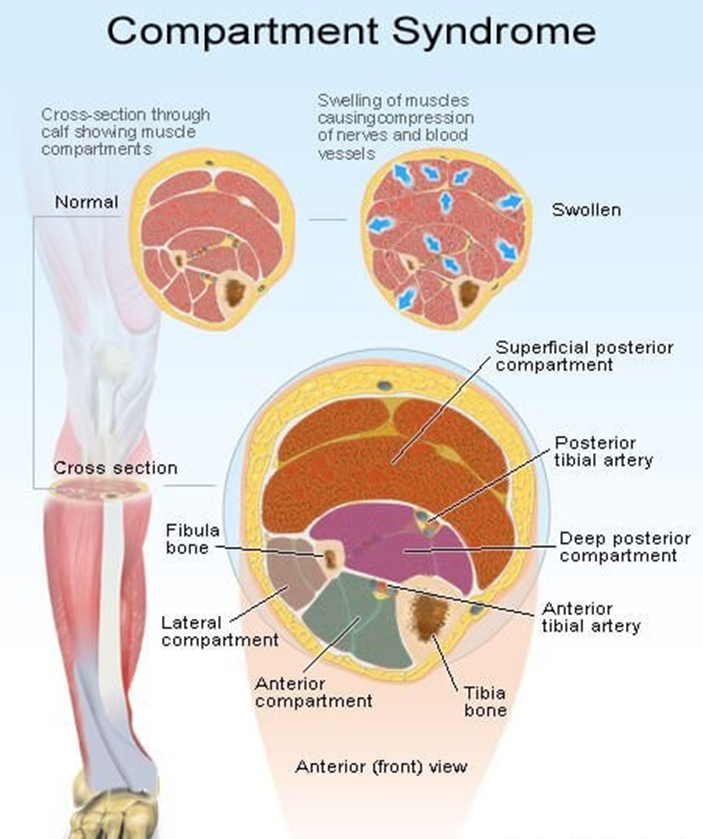
Choice C reason: Bleeding and swelling cause increased pressure in an area that cannot expand is the best response by the nurse. This is the most common cause of compartment syndrome and explains the pathophysiology of the condition. Bleeding and swelling are the result of inflammation and tissue injury that occur after a fracture. They increase the volume of fluid in the compartment, which cannot expand due to the rigid fascia that surrounds it. This leads to increased pressure in the compartment, which compresses the blood vessels, nerves, and muscles and causes ischemia and necrosis of the tissues.
Choice D reason: The fascia expands with injury, causing pressure on underlying nerves and muscles is not the best response by the nurse. This is not a correct statement, as the fascia does not expand with injury. The fascia is a tough connective tissue that encloses the muscle compartments and limits their expansion. The fascia is part of the problem, not the cause, of compartment syndrome. The fascia prevents the compartment from accommodating the increased volume of fluid and causes increased pressure in the compartment.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: Cleansing the skin around the pins is the action that the nurse takes first, because it is the most urgent and relevant action. Cleansing the skin around the pins is a procedure that involves removing any dirt, debris, or secretions from the pin sites, which can help prevent or treat infection, inflammation, or pain. Cleansing the skin around the pins is a priority intervention, as it can reduce the risk of complications, such as osteomyelitis, sepsis, or pin loosening.
Choice B reason: Collecting a culture of the purulent fluid is not the action that the nurse takes first, because it is not the most urgent and relevant action. Collecting a culture of the purulent fluid is a procedure that involves obtaining a sample of the pus from the pin sites and sending it to the laboratory for analysis, which can help identify the type and source of infection. Collecting a culture of the purulent fluid is an important intervention, but it should be done after cleansing the skin around the pins, and with a medical order and a sterile technique.
Choice C reason: Administering an antibiotic is not the action that the nurse takes first, because it is not the most urgent and relevant action. Administering an antibiotic is a procedure that involves giving the client an antimicrobial agent, which can help fight or prevent infection. Administering an antibiotic is an important intervention, but it should be done after cleansing the skin around the pins, and with a medical order and a proper route.
Choice D reason: Instructing the client to complete exercises of the affected extremity is not the action that the nurse takes first, because it is not the most urgent and relevant action. Instructing the client to complete exercises of the affected extremity is a procedure that involves teaching the client how to move and strengthen the muscles and joints of the limb in traction, which can help prevent or treat atrophy, contracture, or thrombosis. Instructing the client to complete exercises of the affected extremity is an important intervention, but it should be done after cleansing the skin around the pins, and with a medical order and a safe technique.
Correct Answer is D
Explanation
Choice A reason: This is not the priority assessment, but it is an important assessment for a client with a femur fracture. Pain is the unpleasant sensation that results from tissue damage or inflammation. Pain can affect the client's physical and psychological wellbeing and interfere with their recovery. The nurse should assess the client's pain level, location, quality, and duration using a valid and reliable pain scale. The nurse should also provide pain relief measures, such as medication, ice, elevation, or distraction, as ordered and as needed.
Choice B reason: This is not the priority assessment, but it is a relevant assessment for a client with a femur fracture. Medication history is the record of the drugs that the client is currently taking or has taken in the past, including prescription, overthecounter, herbal, or recreational drugs. Medication history can help the nurse identify any potential drug interactions, allergies, or contraindications that may affect the client's treatment and recovery. The nurse should ask the client about their medication history and document it accurately and completely.
Choice C reason: This is not the priority assessment, but it is a helpful assessment for a client with a femur fracture. Socioeconomic status is the measure of the client's income, education, occupation, and social class. Socioeconomic status can influence the client's access to health care, ability to afford treatment, compliance with therapy, and support system. The nurse should assess the client's socioeconomic status and provide appropriate referrals, resources, or assistance as needed.
Choice D reason: This is the priority assessment for a client with a femur fracture. Pedal pulses are the pulses that can be felt in the feet, such as the dorsalis pedis or the posterior tibial pulse. Pedal pulses can indicate the blood flow and perfusion to the lower extremities, which can be compromised by a femur fracture. A femur fracture can cause bleeding, swelling, or pressure that can reduce or obstruct the blood supply to the feet, leading to ischemia, necrosis, or gangrene. The nurse should assess the client's pedal pulses regularly and report any changes, such as absent, weak, or thready pulses. The nurse should also monitor the client's skin color, temperature, sensation, and movement in the feet.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today