The nurse is creating an education plan for a client who has a recent diagnosis of Multiple Sclerosis (MS). Which of the following interventions should the nurse include in the client's plan?
Provide total assistance with all ADLs
Order a low-residue diet
Encourage client to void every hour
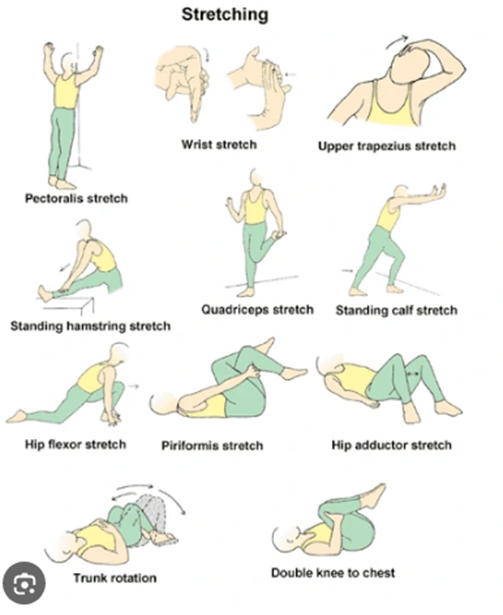
Instruct the client on daily muscle stretching
The Correct Answer is D
Choice A reason: Providing total assistance with all ADLs is not an intervention that should be included in the client's plan. ADLs are activities of daily living, such as bathing, dressing, eating, and toileting. Providing total assistance with all ADLs can reduce the client's independence and self-esteem, and increase their dependence and learned helplessness. The nurse should encourage and assist the client to perform as much as they can by themselves and provide partial or intermittent assistance only when needed.
Choice B reason: Ordering a low-residue diet is not an intervention that should be included in the client's plan. A low-residue diet is a type of diet that limits foods that are high in fiber or indigestible material, such as whole grains, nuts, seeds, fruits, and vegetables. A low-residue diet may be recommended for clients who have inflammatory bowel disease (IBD), diverticulitis, or bowel obstruction, as it can reduce bowel frequency and irritation. However, it is not indicated for clients who have MS, unless they have other comorbidities that require it. A balanced diet that includes adequate fiber, fluids, and nutrients is more beneficial for clients who have MS.
Choice C reason: Encouraging the client to void every hour is not an intervention that should be included in the client's plan. Voiding every hour can be inconvenient and impractical for the client, and may not address their bladder problems effectively. MS can cause bladder dysfunction, such as urinary urgency, frequency, incontinence, or retention, due to nerve damage that affects bladder control. The nurse should assess the type and severity of the bladder dysfunction, and provide appropriate interventions, such as medication, catheterization, pelvic floor exercises, or bladder training.
Choice D reason: Instructing the client on daily muscle stretching is an intervention that should be included in the client's plan. Muscle stretching is a type of exercise that involves extending or elongating a muscle or group of muscles to their full length. Muscle stretching can help prevent or relieve muscle spasticity, stiffness, pain, or contractures that may occur in clients who have MS. The nurse should teach the client how to perform muscle stretching safely and correctly, and encourage them to do it daily or as prescribed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A: Limit fluid intake to prevent incontinence. This is incorrect because limiting fluid intake can lead to dehydration, urinary tract infections, and kidney stones. Fluid intake should be adequate to maintain hydration and flush out bacteria from the urinary tract.
Choice B: Provide regular perineal care to prevent skin breakdown. This is correct because reflex incontinence can cause urine leakage and skin irritation, which can increase the risk of infection and pressure ulcers. Regular perineal care can help keep the skin clean and dry, and prevent complications.
Choice C: Administer hypotonic IV fluids. This is incorrect because hypotonic IV fluids can cause fluid overload, hyponatremia, and cerebral edema. Hypotonic IV fluids are not indicated for clients with reflex incontinence.
Choice D: Teach Kegel exercises to strengthen the pelvic floor. This is incorrect because Kegel exercises are effective for clients with stress or urge incontinence, but not for clients with reflex incontinence. Reflex incontinence is caused by a loss of voluntary control over the bladder due to a spinal cord injury, and Kegel exercises cannot restore this function.
Correct Answer is B
Explanation
Choice A reason: Plantar flexion is the movement of the foot that points the toes downward. It is not a test for gait, but rather a test for muscle strength and nerve function in the lower leg.
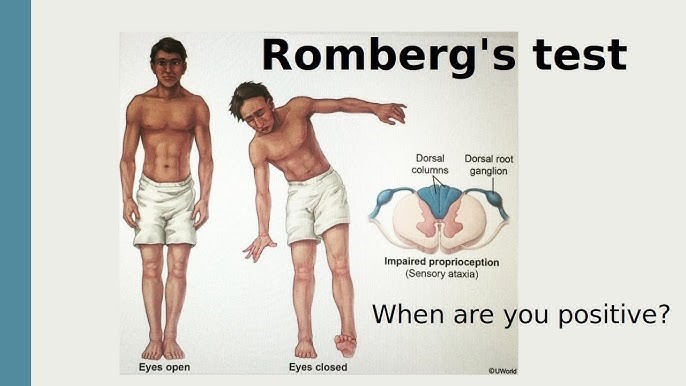
Choice B reason: Romberg is a test for balance and coordination that involves asking the client to stand with their feet together and arms at their sides, first with their eyes open and then with their eyes closed. If the client sways or falls when their eyes are closed, it indicates a problem with their proprioception, which is the sense of position and movement of the body. Ataxia is a condition that affects proprioception and causes impaired gait, so Romberg is an appropriate test for it.
Choice C reason: Achilles reflex is the contraction of the calf muscle when the Achilles tendon is tapped. It is not a test for gait, but rather a test for spinal cord function and nerve damage in the lower leg.
Choice D reason: Patellar reflex is the extension of the lower leg when the patellar tendon is tapped. It is not a test for gait, but rather a test for spinal cord function and nerve damage in the upper leg.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today