A charge nurse is making a room assignment for a client who has scabies. In which of the following rooms should the nurse place the client?
A negative-pressure isolation room
A positive-pressure isolation room
A private room
A semi-private room with a client who has pediculosis capitis
The Correct Answer is C
Choice A reason: A negative-pressure isolation room is not a suitable room for a client who has scabies. A negative-pressure isolation room is used for clients who have airborne infections, such as tuberculosis or chickenpox. It prevents the contaminated air from escaping the room and infecting other people.
Choice B reason: A positive-pressure isolation room is not a suitable room for a client who has scabies. A positive-pressure isolation room is used for clients who have compromised immune systems, such as those undergoing bone marrow transplants or chemotherapy. It prevents the outside air from entering the room and exposing the client to germs.
Choice C reason: A private room is a suitable room for a client who has scabies. Scabies is a skin infection caused by tiny mites that burrow under the skin and cause intense itching and rash. Scabies can spread easily through direct skin-to-skin contact or sharing personal items, such as clothing or bedding. A private room can prevent the transmission of scabies to other clients or staff.
Choice D reason: A semi-private room with a client who has pediculosis capitis is not a suitable room for a client who has scabies. Pediculosis capitis is an infestation of head lice that feeds on human blood and causes itching and irritation on the scalp. Pediculosis capitis can also spread easily through direct contact or sharing personal items, such as combs or hats. Sharing a room with another client who has pediculosis capitis can increase the risk of cross-infection and complicate the treatment of both conditions.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
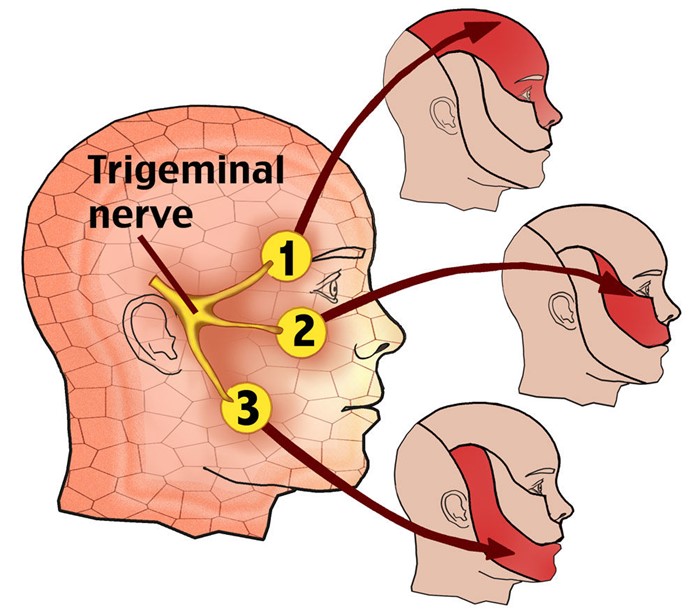
Choice A reason: Analgesics are medications that relieve pain by blocking pain signals or reducing inflammation. They include nonsteroidal anti-inflammatory drugs (NSAIDs), opioids, and acetaminophen. However, analgesics are not very effective in treating trigeminal neuralgia, as they do not address the underlying cause of the pain, which is the compression or irritation of the trigeminal nerve.
Choice B reason: Antihistamines are medications that block the effects of histamine, a chemical that causes allergic reactions such as itching, sneezing, and swelling. They include diphenhydramine, cetirizine, and loratadine. Antihistamines are not effective in treating trigeminal neuralgia, as they do not affect the trigeminal nerve or its function.
Choice C reason: Antibiotics are medications that kill or inhibit the growth of bacteria that cause infections. They include penicillin, amoxicillin, and ciprofloxacin. Antibiotics are not effective in treating trigeminal neuralgia, as they do not target the trigeminal nerve or its pathology.
Choice D reason: Anticonvulsants are medications that prevent or reduce the frequency and severity of seizures by stabilizing the electrical activity of the brain. They include carbamazepine, gabapentin, and phenytoin. Anticonvulsants are the most effective medications in treating trigeminal neuralgia, as they reduce the abnormal firing of the trigeminal nerve that causes the pain. Anticonvulsants are considered the first-line therapy for trigeminal neuralgia and can provide significant relief for most clients.
Correct Answer is A
Explanation
Choice A reason: Giving the patient extra time to perform activities is an appropriate action by the nurse. Bradykinesia is a symptom of Parkinson's disease that causes slow and reduced movement, making it difficult for the patient to initiate and complete tasks. The nurse should respect the patient's autonomy and dignity, and allow them to do as much as they can by themselves, without rushing or interfering.
Choice B reason: Teaching the client to walk more quickly when ambulating is not an appropriate action by the nurse. Bradykinesia can affect the patient's gait and balance, making them prone to falls and injuries. The nurse should not encourage the patient to walk faster than their ability, but rather provide them with assistive devices, such as a cane or walker, and ensure a safe environment.
Choice C reason: Placing the client on a low-protein, low-calorie diet is not an appropriate action by the nurse. Bradykinesia does not require any specific dietary modifications, unless the patient has other comorbidities, such as diabetes or hypertension. The nurse should ensure that the patient has adequate nutrition and hydration, and avoid foods that may interfere with their medication absorption, such as high-fiber or high-fat foods.
Choice D reason: Completing passive range-of-motion exercises daily is not an appropriate action by the nurse. Bradykinesia can cause muscle stiffness and rigidity, which can limit the patient's range of motion and flexibility. The nurse should encourage the patient to do active range-of-motion exercises, which involve moving their own joints to their full extent, rather than passive ones, which involve someone else moving their joints for them. Active exercises can help maintain muscle strength and joint mobility and prevent contractures and deformities.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today