A client is brought to the Emergency Department as one of the first victims of a train accident. The client reports light-headedness, a weak pulse, and uncontrolled bleeding. Which priority tag should a triage nurse use to categorize this client?
Black tag
Red tag
Green tag
Yellow tag
The Correct Answer is B
Choice A reason: A black tag is not the appropriate priority tag for this client, as it indicates that the client is dead or has injuries that are incompatible with life. A black tag is used for clients who have no signs of life, such as pulse, respiration, or pupillary response, or who have severe injuries that cannot be treated with the available resources, such as massive head trauma, decapitation, or incineration. A black tag means that no further care or intervention is provided to the client.
Choice B reason: A red tag is the appropriate priority tag for this client, as it indicates that the client has life-threatening injuries that require immediate attention and treatment. A red tag is used for clients who have compromised airway, breathing, or circulation, such as respiratory distress, shock, severe bleeding, chest pain, or head injury. A red tag means that the client is given the highest priority and is treated as soon as possible.
Choice C reason: A green tag is not the appropriate priority tag for this client, as it indicates that the client has minor injuries that do not require urgent care or intervention. A green tag is used for clients who have stable vital signs and can walk or move without assistance, such as abrasions, sprains, fractures, or minor burns. A green tag means that the client is given the lowest priority and is treated after all other clients.
Choice D reason: A yellow tag is not the appropriate priority tag for this client, as it indicates that the client has serious injuries that require observation and treatment within a short time frame. A yellow tag is used for clients who have potential complications or deterioration of their condition, such as abdominal pain, pelvic injury, open wounds, or spinal injury. A yellow tag means that the client is given the second highest priority and is treated within 30 to 60 minutes.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","E"]
Explanation
Choice A reason: Continuing with the triage process is not an immediate intervention that needs to be taken by the triage nurse, as it may expose more people to the chemical hazard and worsen the situation. The triage nurse should stop the triage process and alert the emergency department staff and management about the potential contamination. The triage nurse should also follow the facility's emergency preparedness plan and protocols for dealing with chemical spills.
Choice B reason: Evacuating the emergency department is an immediate intervention that needs to be taken by the triage nurse, as it helps to protect the safety and health of the staff, clients, and visitors. The triage nurse should assist with evacuating everyone from the emergency department to a safe and designated area, away from the source of contamination. The triage nurse should also ensure that everyone is accounted for and that no one re-enters the emergency department until it is cleared by the authorities.
Choice C reason: Placing the client in a private room is not an immediate intervention that needs to be taken by the triage nurse, as it may not prevent the spread of contamination or provide adequate care to the client. The client who have been exposed to a chemical spill should not be moved to another area of the facility, as they may contaminate other people or surfaces along the way. The client should be kept in a separate and isolated area until they are decontaminated and assessed.
Choice D reason: Treating the client after contaminated items are removed is not an immediate intervention that needs to be taken by the triage nurse, as it may delay or compromise the care of the client. The client who has been exposed to a chemical spill should be treated as soon as possible, as some chemicals can cause serious or irreversible damage to the skin, eyes, lungs, or other organs. The triage nurse should provide basic life support measures, such as airway management, oxygen therapy, or bleeding control while wearing appropriate personal protective equipment (PPE). The triage nurse should also remove any contaminated clothing or jewelry from the client and place them in a sealed bag.
Choice E reason: Sending the client and EMS crew to decontamination is an immediate intervention that needs to be taken by the triage nurse, as it helps to remove or neutralize any harmful chemicals from their skin, hair, or clothing. The triage nurse should direct or escort the client and EMS crew to a designated decontamination area or unit, where they will undergo a thorough washing process with water and soap or other solutions. The triage nurse should also monitor their vital signs and symptoms during and after decontamination.
Correct Answer is B
Explanation
Choice A reason: Plantar flexion is the movement of the foot that points the toes downward. It is not a test for gait, but rather a test for muscle strength and nerve function in the lower leg.
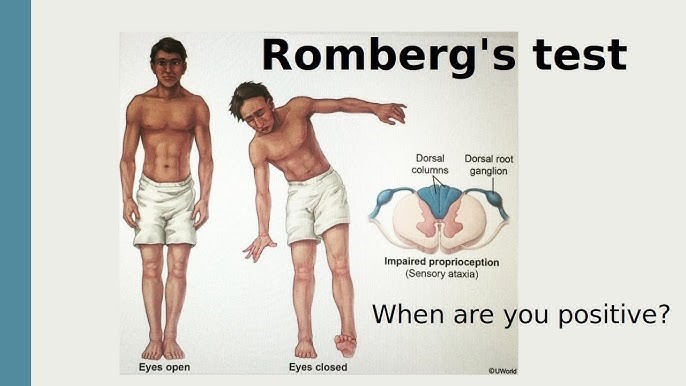
Choice B reason: Romberg is a test for balance and coordination that involves asking the client to stand with their feet together and arms at their sides, first with their eyes open and then with their eyes closed. If the client sways or falls when their eyes are closed, it indicates a problem with their proprioception, which is the sense of position and movement of the body. Ataxia is a condition that affects proprioception and causes impaired gait, so Romberg is an appropriate test for it.
Choice C reason: Achilles reflex is the contraction of the calf muscle when the Achilles tendon is tapped. It is not a test for gait, but rather a test for spinal cord function and nerve damage in the lower leg.
Choice D reason: Patellar reflex is the extension of the lower leg when the patellar tendon is tapped. It is not a test for gait, but rather a test for spinal cord function and nerve damage in the upper leg.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today