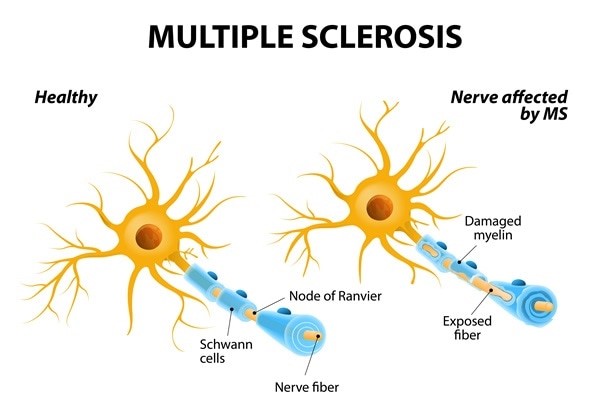
The nurse provides education to a client who is newly diagnosed with multiple sclerosis (MS). Which client statements indicate the need for additional teaching? SELECT ALL THAT APPLY
"I may experience urinary incontinence."
"I should not exercise because this may trigger an exacerbation."
"I should alternate the eye patch every other day to help with the double vision."
"I may experience visual disturbances."
"I need to check the water temperature before I take a bath."
Correct Answer : B,C
Choice A reason: "I may experience urinary incontinence." This statement does not indicate the need for additional teaching. It is a correct statement that reflects an understanding of one of the possible symptoms of MS. Urinary incontinence is caused by nerve damage that affects bladder control.
Choice B reason: "I should not exercise because this may trigger an exacerbation." This statement indicates the need for additional teaching. It is an incorrect statement that reflects a misconception about exercise and MS. Exercise does not cause or worsen MS relapses but rather has many benefits for people with MS, such as improving muscle strength, balance, mobility, mood, and quality of life.
Choice C reason: "I should alternate the eye patch every other day to help with the double vision." This statement indicates the need for additional teaching. It is an incorrect statement that reflects a misunderstanding of how to manage double vision, which is another possible symptom of MS. Alternating the eye patch every other day does not help with double vision, but rather may cause eye fatigue or confusion. The correct way to use an eye patch is to wear it on one eye only when needed, such as when reading or driving.
Choice D reason: "I may experience visual disturbances." This statement does not indicate the need for additional teaching. It is a correct statement that reflects an awareness of another possible symptom of MS. Visual disturbances may include blurred vision, loss of color vision, pain in one eye, or partial or complete blindness.
Choice E reason: "I need to check the water temperature before I take a bath." This statement does not indicate the need for additional teaching. It is a correct statement that reflects a precaution that people with MS should take. Checking the water temperature before taking a bath can prevent burns or scalds, as some people with MS may have reduced sensation or numbness in their skin.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
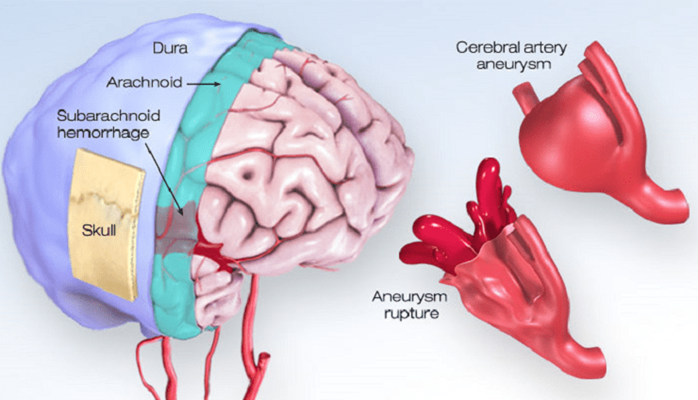
Choice A reason: Gradual onset of several hours is not a manifestation of a hemorrhagic stroke. A hemorrhagic stroke occurs when a blood vessel in the brain bursts, causing bleeding into the surrounding tissue. This usually happens suddenly and without warning, and can cause rapid deterioration of the client's condition.
Choice B reason: Maintains consciousness is not a manifestation of a hemorrhagic stroke. A hemorrhagic stroke can cause increased intracranial pressure, which can compress the brain and impair its function. This can lead to loss of consciousness, coma, or death.
Choice C reason: Sudden severe headache is a manifestation of a hemorrhagic stroke. A hemorrhagic stroke can cause intense pain in the head, neck, or face, due to the pressure and irritation of the bleeding. The headache may be described as "the worst headache of my life" or "thunderclap headache".
Choice D reason: History of neurologic deficits lasting less than 1 hr. is not a manifestation of a hemorrhagic stroke. This is a characteristic of a transient ischemic attack (TIA), which is also known as a mini-stroke. A TIA occurs when a blood clot temporarily blocks an artery in the brain, causing temporary symptoms such as weakness, numbness, vision loss, or speech difficulty. A TIA does not cause permanent damage to the brain, but it is a warning sign of a possible future stroke.
Correct Answer is D
Explanation
Choice A reason: The AP's ability to complete the task without assistance is not one of the five rights of delegation. The nurse is responsible for providing adequate supervision and guidance to the AP, and ensuring that the task is done correctly and safely.
Choice B reason: The AP's ability to prioritize is not one of the five rights of delegation. The nurse is responsible for assigning tasks based on their urgency and importance and communicating clear expectations and deadlines to the AP.
Choice C reason: The AP's rapport with clients is not one of the five rights of delegation. The nurse is responsible for maintaining a therapeutic relationship with clients and respecting their preferences and needs.
Choice D reason: The AP has the knowledge and skill to perform the task is one of the five rights of delegation. The nurse is responsible for assessing the AP's competence and readiness to perform the task, and providing appropriate training and feedback if needed.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today