A nurse is caring for a client with a myocardial infarction. The client questions the need for cardiac rehabilitation since "my heart is already damaged." Which of the following is the appropriate nursing response?
"Diet and exercise is good for you and good for your heart."
"It's not unusual to feel that way at first, but once you learn the routine, you'll enjoy it."
"Cardiac rehabilitation cannot undo the damage to your heart, but it can help you get back to your previous level of activity safely."
"Your doctor is the expert here, and I'm sure he would only recommend what is best for you."
The Correct Answer is C
Choice A reason: "Diet and exercise is good for you and good for your heart." This statement is true, but it is not the appropriate nursing response. It does not address the client's concerns or provide any specific information about cardiac rehabilitation. It may also sound dismissive or patronizing to the client.
Choice B reason: "It's not unusual to feel that way at first, but once you learn the routine, you'll enjoy it." This statement is empathetic, but it is not the appropriate nursing response. It does not explain the purpose or benefits of cardiac rehabilitation. It may also sound unrealistic or optimistic to the client.
Choice C reason: "Cardiac rehabilitation cannot undo the damage to your heart, but it can help you get back to your previous level of activity safely." This statement is the appropriate nursing response. It acknowledges the client's condition and provides factual information about cardiac rehabilitation. It also emphasizes the positive outcomes of cardiac rehabilitation, such as improving physical function, reducing symptoms, and preventing further complications.
Choice D reason: "Your doctor is the expert here, and I'm sure he would only recommend what is best for you." This statement is respectful, but it is not the appropriate nursing response. It does not answer the client's question or provide any education about cardiac rehabilitation. It may also sound evasive or deferential to the client.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
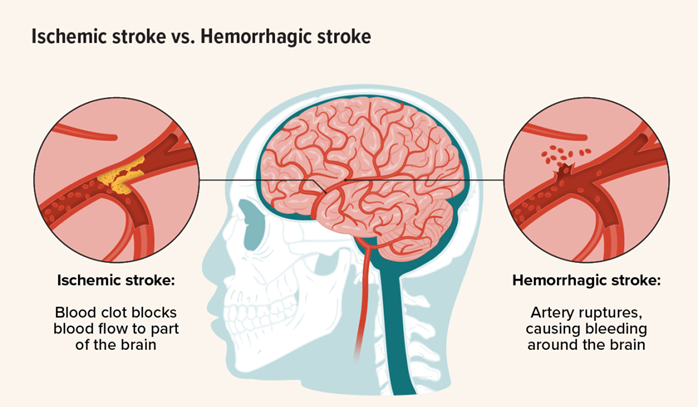
Choice A reason: Monitoring vital signs and neurological status frequently is a priority intervention for a client who has experienced a hemorrhagic stroke, as it helps to detect any changes in the client's condition and guide appropriate treatment. Hemorrhagic stroke is a medical emergency that occurs when a blood vessel in the brain ruptures and causes bleeding into the brain tissue. This can lead to increased intracranial pressure, cerebral edema, and brain damage. Therefore, the nurse should monitor the client's blood pressure, pulse, respiration, temperature, level of consciousness, pupil reaction, motor function, and sensory function frequently and report any abnormalities to the health care provider.
Choice B reason: Maintaining strict bed rest to minimize cerebral blood flow is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may not prevent further bleeding or improve the client's outcome. In fact, strict bed rest may increase the risk of complications such as deep vein thrombosis, pulmonary embolism, pneumonia, pressure ulcers, and muscle atrophy. The nurse should follow the health care provider's orders regarding the client's activity level and position. The nurse should also provide adequate hydration, nutrition, skin care, and comfort measures to the client.
Choice C reason: Administering anticoagulant medications as prescribed is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may worsen the bleeding and increase the risk of intracranial hemorrhage. Anticoagulant medications are used to prevent or treat ischemic stroke, which is caused by a blood clot that blocks a blood vessel in the brain. However, anticoagulant medications are contraindicated in hemorrhagic stroke, as they interfere with the blood's ability to clot and stop the bleeding. The nurse should avoid giving any medications that may affect coagulation or platelet function to the client unless ordered by the health care provider.
Choice D reason: Assisting the client with active range of motion exercises is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may not improve the client's neurological function or prevent complications. Active range of motion exercises are performed by the client with or without assistance from the nurse to maintain joint mobility and muscle strength. However, these exercises are not indicated in the acute phase of hemorrhagic stroke, as they may increase intracranial pressure or cause pain or discomfort to the client. The nurse should consult with the physical therapist before initiating any exercise program for the client.
Correct Answer is C
Explanation
Choice A reason: A skilled nursing facility is a type of long-term care facility that provides 24-hour nursing care and supervision for residents who need assistance with activities of daily living, such as bathing, dressing, eating, and toileting. A skilled nursing facility may not be suitable for a young client with multiple sclerosis who has the potential for improvement and recovery.
Choice B reason: Home care services are a type of community-based care that provides medical and personal care to clients in their own homes. Home care services may include nursing, physical therapy, occupational therapy, speech therapy, social work, or home health aide services. Home care services may be appropriate for a client with multiple sclerosis who has mild to moderate symptoms and a supportive family or caregiver.
Choice C reason: A rehabilitation facility is a type of short-term care facility that provides intensive physical and occupational therapy to clients who have functional impairments due to injury, illness, or surgery. A rehabilitation facility may also provide medical, nursing, and psychological care to clients who need them. A rehabilitation facility may be suitable for a client with multiple sclerosis who has significant muscle weakness and needs to regain strength, mobility, and independence.
Choice D reason: A sub-acute care facility is a type of transitional care facility that provides medical and nursing care to clients who are stable but need complex monitoring or treatment that cannot be provided at home or in a skilled nursing facility. A sub-acute care facility may also provide rehabilitation services to clients who need them. A sub-acute care facility may not be appropriate for a young client with multiple sclerosis who has the potential for improvement and recovery.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today