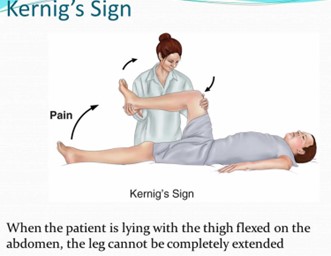
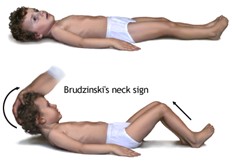
A nurse is assessing a client who reports a severe headache and stiff neck. The nurse's assessment reveals positive Kernig's and Brudzinski's signs. Which of the following actions should the nurse perform first?
Decrease bright lights.
Initiate IV access.
Administer antibiotics.
Implement droplet precautions.
The Correct Answer is D
Choice A reason: Decreasing bright lights is an appropriate action for a nurse to take when caring for a client who has signs of meningitis, as it helps to reduce the photophobia (sensitivity to light) and headache that are common symptoms of the condition. However, this action is not the first priority, as it does not prevent the transmission of the infection or treat the underlying cause.
Choice B reason: Initiating IV access is an appropriate action for a nurse to take when caring for a client who has signs of meningitis, as it facilitates the administration of fluids, medications, and blood products that may be needed to manage the condition. However, this action is not the first priority, as it does not prevent the transmission of the infection or treat the underlying cause.
Choice C reason: Administering antibiotics is an appropriate action for a nurse to take when caring for a client who has signs of meningitis, as it helps to treat the bacterial infection that is the most common cause of the condition. However, this action is not the first priority, as it requires a prescription from the health care provider and confirmation of the diagnosis by laboratory tests such as blood culture or cerebrospinal fluid analysis.
Choice D reason: Implementing droplet precautions is the first priority action for a nurse to take when caring for a client who has signs of meningitis, as it helps to prevent the spread of the infection to other clients and staff members. Droplet precautions are a type of isolation precautions that are used for infections that are transmitted by respiratory droplets, such as meningitis, influenza, and pertussis. Droplet precautions involve wearing a surgical mask when entering the client's room, placing the client in a private room or cohorting with other clients who have the same infection, and limiting visitors and staff contact with the client.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: Scheduling energy-intensive activities at the time of day when the client has higher energy levels is the best activity plan for conserving the client's energy without compromising physical or mental health, as it allows the client to perform the tasks that require more effort and endurance when they feel more alert and capable. This can help the client to avoid fatigue, frustration, and injury, and to achieve their goals more effectively. The nurse should assess the client's individual preferences and patterns of energy fluctuation, and help them to prioritize and plan their activities accordingly.
Choice B reason: Scheduling all activities within a small block of time to allow the client a longer, uninterrupted rest period is not a good activity plan for conserving the client's energy without compromising physical or mental health, as it may cause the client to overexert themselves and deplete their energy reserves. This can lead to exhaustion, pain, and stress, and impair the client's recovery and quality of life. The nurse should advise the client to balance their activities with adequate rest periods throughout the day and to avoid doing too much or too little at once.
Choice C reason: Scheduling toilet breaks before and after any other planned activity is not a good activity plan for conserving the client's energy without compromising physical or mental health, as it may not be realistic or feasible for some clients. Some clients may have urinary or bowel problems that require them to use the toilet more frequently or urgently, such as incontinence, infection, or constipation. Forcing them to follow a rigid schedule may cause them discomfort, embarrassment, or complications. The nurse should assess the client's elimination needs and habits, and help them to manage their toileting needs in a comfortable and convenient way.
Choice D reason: Scheduling the client's hygiene activities and limiting visitors is not a good activity plan for conserving the client's energy without compromising physical or mental health, as it may neglect the client's social and emotional needs. Hygiene activities are important for maintaining the client's physical health and well-being, but they can also be tiring and challenging for some clients. Limiting visitors may reduce the noise and stimulation in the environment, but it can also isolate the client from their family and friends who can provide support and companionship. The nurse should assist the client with their hygiene needs as needed, and encourage them to interact with their visitors as tolerated.
Correct Answer is A
Explanation
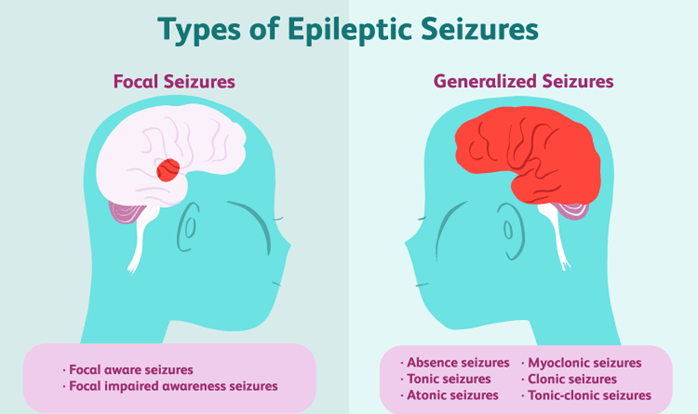
Choice A reason: "Move objects away from the client." This instruction should be included in the teaching. It is a safety measure that can prevent injury or harm to the client during a seizure. Moving objects away from the client can create more space and avoid contact with sharp, hard, or hot items.
Choice B reason: "Restrain the client." This instruction should not be included in the teaching. It is a harmful action that can worsen or prolong the seizure. Restraining the client can interfere with their natural movements, cause pain or discomfort, or damage their muscles or joints.
Choice C reason: "Place the client on his back." This instruction should not be included in the teaching. It is a dangerous position that can compromise the client's airway and breathing. Placing the client on his back can increase the risk of choking, aspiration, or suffocation.
Choice D reason: "Insert a padded tongue blade into the client's mouth." This instruction should not be included in the teaching. It is an outdated and ineffective practice that can cause more harm than good. Inserting a padded tongue blade into the client's mouth can damage their teeth, gums, tongue, or lips, or block their airway. Contrary to popular belief, it is impossible for a person to swallow their tongue during a seizure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today