A nurse is caring for a client who has experienced a hemorrhagic stroke. Which intervention should the nurse prioritize when providing care to the client?
Monitoring vital signs and neurological status frequently.
Maintaining strict bed rest to minimize cerebral blood flow.
Administering anticoagulant medications as prescribed.
Assisting the client with active range of motion exercises.
The Correct Answer is A
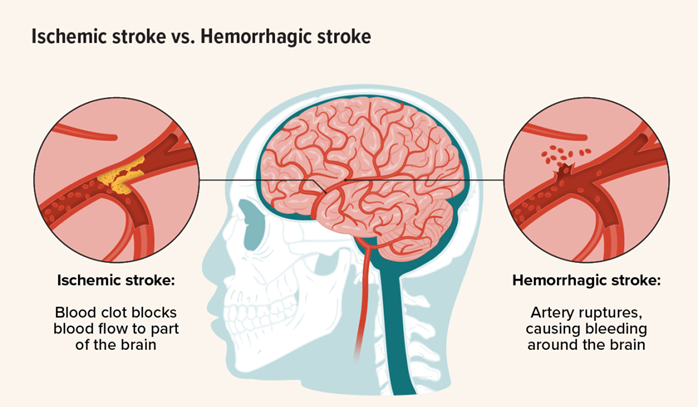
Choice A reason: Monitoring vital signs and neurological status frequently is a priority intervention for a client who has experienced a hemorrhagic stroke, as it helps to detect any changes in the client's condition and guide appropriate treatment. Hemorrhagic stroke is a medical emergency that occurs when a blood vessel in the brain ruptures and causes bleeding into the brain tissue. This can lead to increased intracranial pressure, cerebral edema, and brain damage. Therefore, the nurse should monitor the client's blood pressure, pulse, respiration, temperature, level of consciousness, pupil reaction, motor function, and sensory function frequently and report any abnormalities to the health care provider.
Choice B reason: Maintaining strict bed rest to minimize cerebral blood flow is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may not prevent further bleeding or improve the client's outcome. In fact, strict bed rest may increase the risk of complications such as deep vein thrombosis, pulmonary embolism, pneumonia, pressure ulcers, and muscle atrophy. The nurse should follow the health care provider's orders regarding the client's activity level and position. The nurse should also provide adequate hydration, nutrition, skincare, and comfort measures to the client.
Choice C reason: Administering anticoagulant medications as prescribed is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may worsen the bleeding and increase the risk of intracranial hemorrhage. Anticoagulant medications are used to prevent or treat ischemic stroke, which is caused by a blood clot that blocks a blood vessel in the brain. However, anticoagulant medications are contraindicated in hemorrhagic stroke, as they interfere with the blood's ability to clot and stop the bleeding. The nurse should avoid giving any medications that may affect coagulation or platelet function to the client unless ordered by the health care provider.
Choice D reason: Assisting the client with active range of motion exercises is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may not improve the client's neurological function or prevent complications. Active range of motion exercises are performed by the client with or without assistance from the nurse to maintain joint mobility and muscle strength. However, these exercises are not indicated in the acute phase of hemorrhagic stroke, as they may increase intracranial pressure or cause pain or discomfort to the client. The nurse should consult with the physical therapist before initiating any exercise program for the client.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: A negative-pressure isolation room is not a suitable room for a client who has scabies. A negative-pressure isolation room is used for clients who have airborne infections, such as tuberculosis or chickenpox. It prevents the contaminated air from escaping the room and infecting other people.
Choice B reason: A positive-pressure isolation room is not a suitable room for a client who has scabies. A positive-pressure isolation room is used for clients who have compromised immune systems, such as those undergoing bone marrow transplants or chemotherapy. It prevents the outside air from entering the room and exposing the client to germs.
Choice C reason: A private room is a suitable room for a client who has scabies. Scabies is a skin infection caused by tiny mites that burrow under the skin and cause intense itching and rash. Scabies can spread easily through direct skin-to-skin contact or sharing personal items, such as clothing or bedding. A private room can prevent the transmission of scabies to other clients or staff.
Choice D reason: A semi-private room with a client who has pediculosis capitis is not a suitable room for a client who has scabies. Pediculosis capitis is an infestation of head lice that feeds on human blood and causes itching and irritation on the scalp. Pediculosis capitis can also spread easily through direct contact or sharing personal items, such as combs or hats. Sharing a room with another client who has pediculosis capitis can increase the risk of cross-infection and complicate the treatment of both conditions.
Correct Answer is A
Explanation
Choice A reason: Monitoring vital signs and neurological status frequently is a priority intervention for a client who has experienced a hemorrhagic stroke, as it helps to detect any changes in the client's condition and guide appropriate treatment. Hemorrhagic stroke is a medical emergency that occurs when a blood vessel in the brain ruptures and causes bleeding into the brain tissue. This can lead to increased intracranial pressure, cerebral edema, and brain damage. Therefore, the nurse should monitor the client's blood pressure, pulse, respiration, temperature, level of consciousness, pupil reaction, motor function, and sensory function frequently and report any abnormalities to the health care provider.
Choice B reason: Maintaining strict bed rest to minimize cerebral blood flow is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may not prevent further bleeding or improve the client's outcome. In fact, strict bed rest may increase the risk of complications such as deep vein thrombosis, pulmonary embolism, pneumonia, pressure ulcers, and muscle atrophy. The nurse should follow the health care provider's orders regarding the client's activity level and position. The nurse should also provide adequate hydration, nutrition, skin care, and comfort measures to the client.
Choice C reason: Administering anticoagulant medications as prescribed is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may worsen the bleeding and increase the risk of intracranial hemorrhage. Anticoagulant medications are used to prevent or treat ischemic stroke, which is caused by a blood clot that blocks a blood vessel in the brain. However, anticoagulant medications are contraindicated in hemorrhagic stroke, as they interfere with the blood's ability to clot and stop the bleeding. The nurse should avoid giving any medications that may affect coagulation or platelet function to the client unless ordered by the health care provider.
Choice D reason: Assisting the client with active range of motion exercises is not a priority intervention for a client who has experienced a hemorrhagic stroke, as it may not improve the client's neurological function or prevent complications. Active range of motion exercises are performed by the client with or without assistance from the nurse to maintain joint mobility and muscle strength. However, these exercises are not indicated in the acute phase of hemorrhagic stroke, as they may increase intracranial pressure or cause pain or discomfort to the client. The nurse should consult with the physical therapist before initiating any exercise program for the client.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today