A client with myasthenia gravis has lost 6 kg of weight over the last 2 months. What should the nurse suggest to improve this client's nutritional status?
Plan medication doses to occur before meals
Restrict drinking fluids before and during meals
Increase the amount of fat and carbohydrates in meals
Eat three large meals per day
The Correct Answer is A
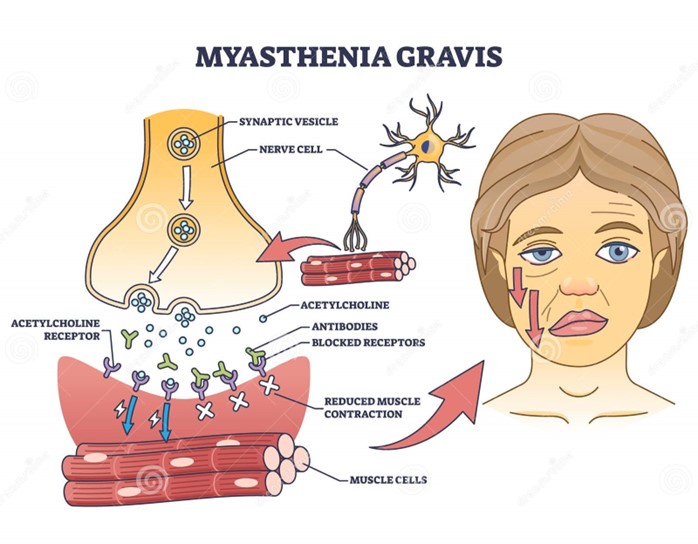
Choice A reason: Planning medication doses to occur before meals is a good suggestion to improve the client's nutritional status. Myasthenia gravis is a neuromuscular disorder that causes weakness and fatigue of the voluntary muscles, especially those involved in chewing and swallowing. Taking anticholinesterase medications before meals can enhance muscle strength and coordination, and make it easier for the client to eat and avoid choking or aspiration.
Choice B reason: Restricting drinking fluids before and during meals is not a good suggestion to improve the client's nutritional status. Fluid intake is important for hydration and digestion, and should not be limited unless there is a medical reason, such as fluid overload or heart failure. Drinking fluids before and during meals can also help lubricate the food and prevent dryness or irritation of the mouth and throat.
Choice C reason: Increasing the amount of fat and carbohydrates in meals is not a good suggestion to improve the client's nutritional status. Fat and carbohydrates are sources of energy, but they can also increase the risk of obesity, diabetes, or cardiovascular disease if consumed excessively. A balanced diet that includes adequate protein, vitamins, minerals, and fiber is more beneficial for the client's health and well-being.
Choice D reason: Eating three large meals per day is not a good suggestion to improve the client's nutritional status. Eating large meals can be difficult and exhausting for the client with myasthenia gravis, as their muscle strength and endurance may decline over time. Eating smaller and more frequent meals can help maintain the energy level and prevent fatigue or hunger.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","D","E"]
Explanation
Choice A reason: Initiating a plan of care for a client who is postoperative from an appendectomy is not a task that the RN should delegate to the LPN, as it requires nursing judgment, critical thinking, and assessment skills that are beyond the scope of practice of the LPN. The RN is responsible for developing, implementing, and evaluating the plan of care for each client based on their individual needs, preferences, and goals. The RN can delegate some aspects of the plan of care to the LPN, such as performing routine tasks or monitoring the client's status, but the RN must supervise and evaluate the LPN's performance.
Choice B reason: Administering a tap-water enema to a client who is preoperative is a task that the RN can delegate to the LPN, as it is a standardized procedure that does not require nursing judgment or assessment. The LPN has the knowledge and skills to perform this task safely and effectively, following the established policies and protocols of the facility. The RN should provide clear instructions and expectations to the LPN, such as the type, amount, and temperature of the solution, the position and comfort of the client, and the signs and symptoms to report. The RN should also verify that the LPN has completed the task and documented the outcome.
Choice C reason: Providing discharge instructions to a confused client's spouse is not a task that the RN should delegate to the LPN, as it involves teaching, counseling, and evaluating the client's and family's understanding and readiness for discharge. These are complex activities that require nursing judgment, communication skills, and evaluation skills that are beyond the scope of practice of the LPN. The RN is responsible for ensuring that the client and family receive adequate information and education about the client's condition, treatment, medications, follow-up care, and community resources. The RN can delegate some aspects of discharge planning to the LPN, such as collecting data or providing reinforcement of teaching, but the RN must supervise and evaluate the LPN's performance.
Choice D reason: Catheterizing a client who has not voided in 8 hours is a task that the RN can delegate to the LPN, as it is a standardized procedure that does not require nursing judgment or assessment. The LPN has the knowledge and skills to perform this task safely and effectively, following the established policies and protocols of the facility. The RN should provide clear instructions and expectations to the LPN, such as the type and size of the catheter, the sterile technique, and the urine output measurement. The RN should also verify that the LPN has completed the task and documented the outcome.
Choice E reason: Obtaining vital signs from a client who is 6 hours postoperative is a task that the RN can delegate to the LPN, as it is a routine task that does not require nursing judgment or assessment. The LPN has the knowledge and skills to perform this task safely and effectively, using appropriate equipment and techniques. The RN should provide clear instructions and expectations to the LPN, such as the frequency and parameters of vital signs monitoring. The RN should also verify that the LPN has completed the task and documented the outcome.
Correct Answer is D
Explanation
Choice A reason: A public health nurse is a nurse who works to improve the health and well-being of populations and communities, not specific workplaces. A public health nurse may focus on disease prevention, health promotion, environmental health, or emergency preparedness.
Choice B reason: A community nurse specialist is a nurse who has advanced education and training in a specific area of nursing practice, such as gerontology, oncology, or mental health. A community nurse specialist may work in various settings, such as hospitals, clinics, or schools, to provide specialized care and education to clients and families.
Choice C reason: A nurse clinician is a nurse who has expertise in clinical practice, research, and education. A nurse clinician may work in academic or clinical settings, such as universities, hospitals, or research centers, to develop and implement evidence-based practices and policies.
Choice D reason: An occupational health nurse is a nurse who works to protect and promote the health and safety of workers in various industries, such as manufacturing, mining, or construction. An occupational health nurse may provide services such as health assessment, injury prevention, emergency response, or wellness programs.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today