A patient with fluid overload is prescribed furosemide (Lasix) 20 mg by mouth each day. What should the nurse include when teaching the patient about this medication? (Select all that apply.)
Measure body weight every day.
Expect urination to increase.
Take the medication before going to sleep.
Report swelling of the face or hands.
Expect to feel weak and dizzy.
Correct Answer : A,B,D,E
Choice A: Measure body weight every day is correct because body weight is an indicator of fluid balance and can help monitor the effectiveness of the medication. The nurse should instruct the patient to weigh themselves at the same time each day, preferably in the morning, and report any significant changes to the provider.
Choice B: Expect urination to increase is correct because furosemide is a diuretic that works by blocking the reabsorption of sodium and water in the kidneys, thus increasing urine output and reducing fluid volume. The nurse should instruct the patient to drink enough fluids to prevent dehydration and electrolyte imbalance and to avoid taking the medication at night to prevent nocturia and sleep disturbance.
Choice C: Taking the medication before going to sleep is incorrect because taking furosemide at night can cause nocturia and sleep disturbance, as well as increase the risk of falls. The nurse should instruct the patient to take the medication in the morning or early afternoon and to avoid caffeine and alcohol, which can also increase urination.
Choice D: Report swelling of the face or hands is correct because swelling of the face or hands can indicate an allergic reaction or angioedema, which are rare but serious side effects of furosemide. The nurse should instruct the patient to stop taking the medication and seek immediate medical attention if they experience swelling of the face or hands, as well as difficulty breathing, hives, or itching.
Choice E: Expecting to feel weak and dizzy is correct because weakness and dizziness are common side effects of furosemide, especially when starting or increasing the dose. The nurse should instruct the patient to rise slowly from a sitting or lying position and to use caution when driving or performing other activities that require alertness. The nurse should also instruct the patient to report any signs of hypotension, such as fainting, blurred vision, or chest pain.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","D","E"]
Explanation
Choice A: Limit intake of canned soups is correct because canned soups are high in sodium and can increase blood pressure and fluid retention. The nurse should advise the client to choose low-sodium or homemade soups instead.
Choice B: Choose botled salad dressings is incorrect because botled salad dressings are also high in sodium and can have added sugars and fats. The nurse should advise the client to make their own salad dressings with vinegar, oil, herbs, and spices.
Choice C: Choose diet sodas over botled water is incorrect because diet sodas are not a healthy alternative to water. Diet sodas contain artificial sweeteners, caffeine, and phosphoric acid, which can affect the body's pH balance and calcium absorption. The nurse should advise the client to drink plain water or flavored water with natural ingredients.
Choice D: Replace processed meats with fresh meat products is correct because processed meats such as bacon, ham, sausage, and hot dogs are high in sodium and preservatives. The nurse should advise the client to choose fresh meat products such as chicken, turkey, fish, or lean beef.
Choice E: Read labels on foods before eating is correct because reading labels can help the client identify the sodium content and other ingredients in foods. The nurse should advise the client to look for foods that have less than 140 mg of sodium per serving and avoid foods that have salt, sodium, or monosodium glutamate (MSG) in the ingredient list.
Correct Answer is C
Explanation
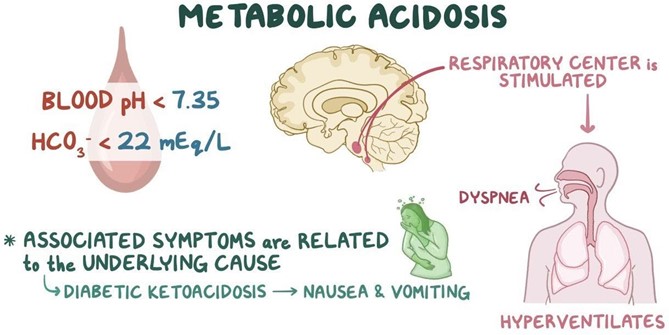
Choice A: Metabolic acidosis is incorrect because it is characterized by a low pH and a low HCO3, not a high PaCO2. Metabolic acidosis occurs when there is an excess of metabolic acids in the body, such as lactic acid, ketoacids, or salicylates.
Choice B: Respiratory alkalosis is incorrect because it is characterized by a high pH and a low PaCO2, not a low pH and a high PaCO2. Respiratory alkalosis occurs when there is excessive loss of carbon dioxide through hyperventilation, such as in anxiety, fever, or aspirin overdose.
Choice C: Respiratory acidosis is correct because it is characterized by a low pH and a high PaCO2. Respiratory acidosis occurs when there is impaired gas exchange or hypoventilation, resulting in accumulation of carbon dioxide in the blood. This can be caused by conditions such as chronic obstructive pulmonary disease (COPD), pneumonia, asthma, or chest trauma.
Choice D: Metabolic alkalosis is incorrect because it is characterized by a high pH and a high HCO3, not a low pH and a high PaCO2. Metabolic alkalosis occurs when there is a loss of metabolic acids or an excess of bicarbonate in the body, such as from vomiting, gastric suctioning, or diuretic therapy.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today