A nurse is teaching a hypertensive client who is taking hydrochlorothiazide. What client statement indicates understanding about hydrochlorothiazide?
"I will not take this medicine when my blood pressure is okay"
"I will check blood pressure in both arms and legs before taking the drug."
"I will decrease potassium foods such as bananas in my diet."
"I will take this medication in the morning since I will be urinating more."
The Correct Answer is D
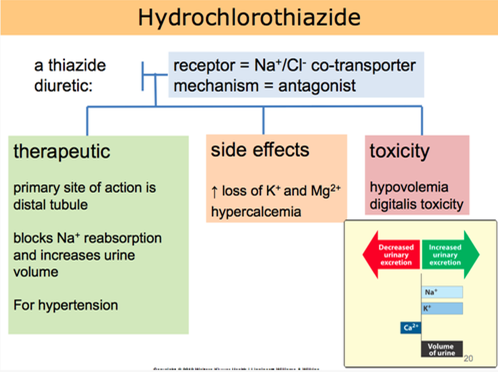
Hydrochlorothiazide is a diuretic medication commonly prescribed for hypertension. It works by increasing urine output, which helps to reduce fluid volume and lower blood pressure. Taking the medication in the morning is beneficial because the increased urine production during the day can help prevent nighttime disruptions due to frequent urination.
Let's go through the other statements and explain why they are not accurate:
"I will not take this medicine when my blood pressure is okay":
This statement indicates a misunderstanding about the purpose of hydrochlorothiazide. It is important to take prescribed medications consistently, even when blood pressure readings are within the normal range, as they are intended to help maintain blood pressure control.
"I will check blood pressure in both arms and legs before taking the drug":
Checking blood pressure in both arms and legs is not directly related to hydrochlorothiazide use. Blood pressure should be monitored regularly, but it is not necessary to perform these measurements specifically before taking the medication.
"I will decrease potassium foods such as bananas in my diet":
Hydrochlorothiazide can cause potassium loss as a side effect. However, reducing potassium-rich foods without healthcare provider guidance may not be appropriate. It is important for the client to discuss dietary adjustments and potassium supplementation with their healthcare provider if needed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Among the given findings, the most important finding to report to the health care provider in a client with a hypertensive emergency is the new-onset blurry vision and facial asymmetry. These symptoms may indicate that the client is experiencing a hypertensive crisis with potential complications such as hypertensive encephalopathy or stroke.
Blurred vision and facial asymmetry are concerning neurological symptoms that suggest possible damage to the blood vessels or organs in the brain. It is crucial to notify the health care provider immediately so that appropriate interventions can be initiated to address the underlying cause and prevent further complications.
While the other findings may also be associated with elevated blood pressure, the new-onset blurry vision and facial asymmetry indicate possible neurological involvement and require immediate attention. Headache, epistaxis (nosebleed), and decreased urine output may be significant symptoms, but the potential neurological implications make the new-onset blurry vision and facial asymmetry the priority for reporting.
Correct Answer is A
Explanation
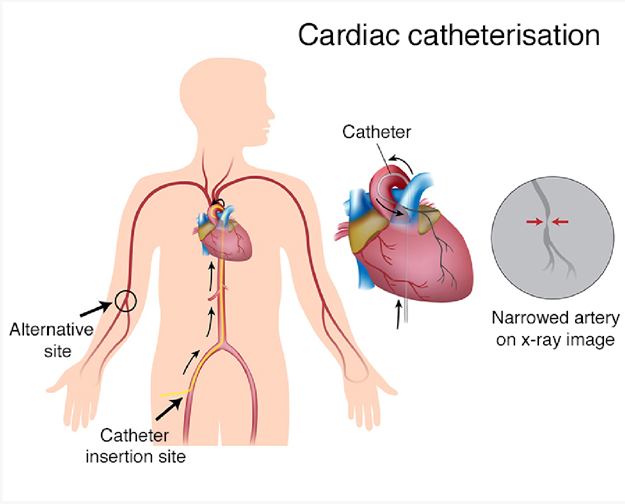
ST-segment elevation during exercise stress testing is a concerning finding that may indicate reduced blood flow to the heart muscle. It can be a sign of myocardial ischemia or coronary artery disease. Cardiac catheterization is a diagnostic procedure that allows direct visualization of the coronary arteries and helps identify any blockages or narrowing that may be causing the ST-segment elevation.
Here's an explanation of why the other options are not the most appropriate procedures:
Transesophageal echocardiogram: Transesophageal echocardiogram (TEE) is a diagnostic test that involves inserting a probe into the esophagus to obtain detailed images of the heart. It is not typically used to evaluate ST-segment elevation, which primarily indicates coronary artery issues rather than structural abnormalities.
Telemetry monitoring: Telemetry monitoring involves continuous monitoring of a patient's heart rhythm and can be used for various cardiac conditions. While telemetry monitoring may be necessary for ongoing cardiac assessment, it is not a specific procedure to address the ST-segment elevation found during the exercise stress test.
Pharmacologic stress test: A pharmacologic stress test is an alternative to an exercise stress test for patients who cannot exercise. It involves administering medications that stimulate the heart to mimic the effects of exercise. While a pharmacologic stress testcan also reveal ST-segment changes, the presence of ST-segment elevation usually requires further evaluation with a more invasive procedure like cardiac catheterization.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today