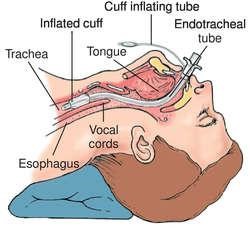
A nurse is suctioning the airway of a client who is receiving mechanical ventilation via an endotracheal tube. Which of the following findings should the nurse identify as an indication that the suctioning has been effective?
Thinning of mucous secretions
Decreased peak inspiratory pressure
Presence of a productive cough
Flattening of the artificial airway cuff
The Correct Answer is B
Choice A reason
While thinning of secretions can be a positive sign, it's not always visible. A decrease in peak inspiratory pressure is a more objective indicator of improved airway patency.
Choice B reason.
Peak inspiratory pressure is the maximum pressure required to push air into the lungs. If suctioning is effective, it will remove secretions and reduce airway resistance, leading to a decrease in peak inspiratory pressure.
Choice C reason:
While a productive cough can indicate that secretions are being moved, it doesn't directly measure the effectiveness of suctioning.
Choice D reason:
Flattening of the artificial airway cuff: Flattening of the artificial airway cuff is not a relevant indicator of the effectiveness of suctioning. The cuff of an endotracheal tube is inflated to prevent air leaks around the tube and to maintain proper ventilation. It is not directly related to the effectiveness of suctioning.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason:
Discourage physical activity during the day is incorrect. Encouraging physical activity is generally beneficial for individuals with dementia. Regular exercise can improve mood, reduce agitation, and enhance overall health. However, the level and type of physical activity should be tailored to the individual's abilities and preferences.
Choice B reason
Use clothing with buttons and zippers is incorrect. Clothing with buttons and zippers can be challenging for individuals with dementia due to fine motor skill impairments and difficulty with dressing. It is often recommended to use clothing with simple closures, such as Velcro or elastic bands, to make dressing easier and more manageable for the individual.
Choice C reason:
Individuals with dementia may experience difficulties with communication, memory, and problem-solving, which can affect their ability to recognize and express the need to use the restroom. As a result, they may be at risk of urinary or bowel incontinence. To address this concern and promote the client's comfort and dignity, establishing a toileting schedule is essential. A consistent routine for bathroom breaks can help prevent accidents and improve the client's overall well-being.
Choice D reason:
Engage the client in activities that increase sensory stimulation is incorrect. While sensory stimulation activities can be enjoyable and engaging for individuals with dementia, it is essential to select activities that are appropriate and not overwhelming. Some individuals with dementia may become overstimulated, which can lead to agitation or distress. Activities should be tailored to the individual's preferences and abilities.
Correct Answer is B
Explanation
A. "Perhaps you think the ECT is dangerous, but I've seen it have good results." This response is dismissive of the client's concerns and implies that the nurse knows better than the client.
B. "You have the right to change your mind about this procedure at any time." This response respects the client's autonomy and informs them of their rights.
C. "Everyone gets a little nervous about this procedure as the time for it approaches." This response minimizes the client's feelings and assumes that they are experiencing normal anxiety.
D. "Your doctor wouldn't have suggested ECT if they didn't think it would help you." This response shifts the responsibility to the doctor and does not address the client's fears.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today