A nurse is caring for a client who has immunosuppression and a continuous IV infusion.
Which of the following actions should the nurse take?
Assess the client's IV site every 8 hr.
Check the client's WBC count every 48 hr.
Monitor the client's mouth every 8 hr.
Change the client's IV tubing every 48 hr.
The Correct Answer is C
- A. Incorrect. The nurse should assess the client's IV site every hour to prevent infection and phlebitis.
- B. Incorrect. The nurse should check the client's WBC count every day to monitor for signs of infection or bone marrow suppression.
- C. Correct. The nurse should monitor the client's mouth every 8 hr for signs of oral candidiasis, which is a common fungal infection in immunosuppressed clients.\
- D. Incorrect. The nurse should change the client's IV tubing every 24 hr to reduce the risk of bacterial contamination.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Droplet.
The rationale for each choice is as follows:
- A. Droplet: Correct. Pneumonia is transmitted by respiratory droplets that are generated by coughing, sneezing, or talking. The nurse should wear a surgical mask and eye protection when caring for the client and maintain a distance of at least 3 feet from the client.
- B. Airborne: Incorrect. Airborne precautions are used for diseases that are transmitted by small particles that remain suspended in the air for long periods of time, such as tuberculosis, measles, or chickenpox. The nurse should wear a respirator and place the client in a negative-pressure room.
- C. Contact: Incorrect. Contact precautions are used for diseases that are transmitted by direct or indirect contact with the client or the client's environment, such as Clostridium difficile, scabies, or MRSA. The nurse should wear gloves and a gown and use dedicated equipment for the client.
- D. Protective environment: Incorrect. Protective environment precautions are used for clients who are immunocompromised and at risk of infection from others, such as clients who have had a stem cell transplant or are receiving chemotherapy. The nurse should wear a mask, gloves, and a gown and place the client in a positive-pressure room with HEPA filtration.
Correct Answer is C
Explanation
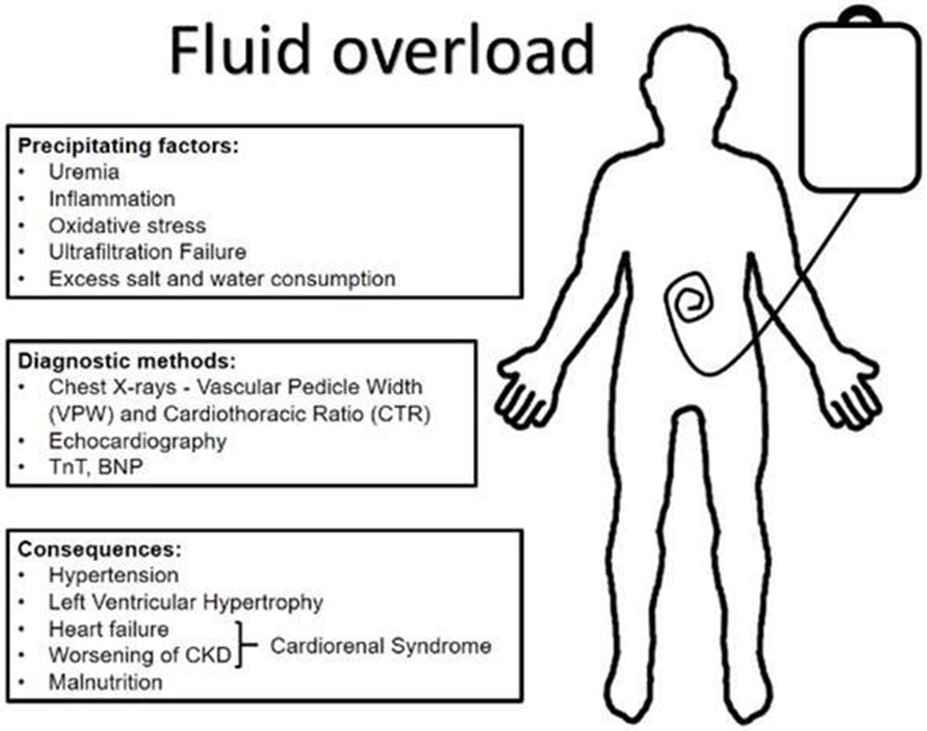
- A. Oliguria. This is incorrect because oliguria, or decreased urine output, is a sign of fluid volume deficit, not fluid volume overload.
- B. Bradycardia. This is incorrect because bradycardia, or slow heart rate, is not a typical sign of fluid volume overload, unless the client has a cardiac condition that affects the heart's response to fluid overload.
- C. Dyspnea. This is correct because dyspnea, or difficulty breathing, is a common sign of fluid volume overload, as excess fluid accumulates in the lungs and impairs gas exchange.
- D. Poor skin turgor. This is incorrect because poor skin turgor, or decreased elasticity of the skin, is a sign of dehydration, not fluid volume overload.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today