A nurse is preparing to administer a liquid medication to a 6-month-old infant who is crying. Which of the
following actions should the nurse take to reduce the risk of aspiration?
Pinch the infant's nares during administration
Administer the whole dose at once
Hold the infant in a side-lying position
Administer using a needleless syringe in the buccal cavity
The Correct Answer is D
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Correct answer: C
A) Start the first patch on the seventh day of the menstrual cycle: The patch is typically applied on the first day of the menstrual cycle or the first Sunday after the menstrual period begins, not on the seventh day. This helps ensure effective contraception from the start of use.
B) The contraceptive effect will continue for 6 months following discontinuation of the medication: The contraceptive effect of the patch does not last for 6 months after discontinuation. Once the patch is removed and not replaced, hormone levels drop, and fertility can return relatively quickly, typically within a few days to weeks.
C) Apply the patch to the lower abdomen: The patch should be applied to clean, dry, and intact skin on areas such as the lower abdomen, upper outer arm, buttock, or upper torso (excluding the breasts). This location allows for consistent hormone absorption.
D) Expect to have a headache during the first month: While some individuals may experience headaches as a side effect of hormonal contraceptives, this is not an expected or guaranteed outcome. Any persistent or severe headache should be reported to the healthcare provider, as it could indicate other concerns.
Correct Answer is C
Explanation
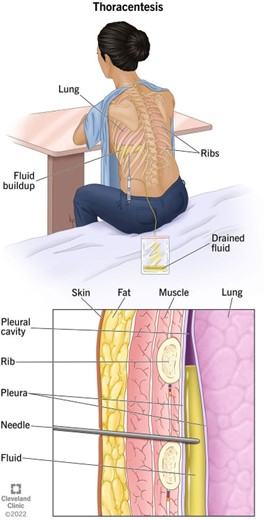
c. "I will have a chest x-ray following the procedure."
Explanation:
The statement that indicates an understanding of the information provided is "I will have a chest x-ray following the procedure."
Explanation for the other options:
a. "I will have general anesthesia during the procedure":
This statement is incorrect. Thoracentesis is typically performed using local anesthesia, which numbs the area where the needle will be inserted. General anesthesia, which induces a state of unconsciousness, is not usually required for this procedure.
b. "I will lie flat for 6 hours following the procedure":
This statement is incorrect. While the client may be advised to lie still for a short period after the thoracentesis, it is not necessary for them to lie flat for a full 6 hours. The specific post-procedure instructions may vary depending on the client's condition and the healthcare provider's preferences.
d. "I will breathe deeply through my nose during the procedure":
This statement is incorrect. During a thoracentesis, the client is typically asked to sit upright and lean forward to allow beter access to the space between the lungs and chest wall. They may be instructed to take slow, deep breaths and hold their breath for short periods as needed during the procedure to help maintain proper positioning and reduce the risk of complications.
In summary, the statement that demonstrates an understanding of the thoracentesis procedure is "I will have a chest x-ray following the procedure." This indicates the client's awareness of the need for a post- procedure chest x-ray to evaluate the results and ensure the absence of any complications.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today