A nurse is educating the family of an adolescent client with anorexia nervosa about the issues surrounding this eating disorder. Which statement made by the parent indicates that the education is effective?
"The behavior our child exhibits, such as not eating, are ways that allow our child to feel control."
"This is a phase our child is going through, and when they get hungry enough, they will eat."
"Our child must be having some problems identifying their sexual identity, and this is how it is expressed."
"We have a codependent relationship with our child and enable the behaviors exhibited."
The Correct Answer is D
Choice A reason: This statement reflects a partial understanding of the control issues associated with anorexia but does not indicate a full understanding of the disorder's complexity or the family's role in recovery.
Choice B reason: This statement suggests a lack of understanding of anorexia nervosa, as it is not a phase but a serious mental health condition that requires professional treatment.
Choice C reason: While issues with sexual identity can be stressful, they are not typically the cause of anorexia nervosa, which is characterized by an intense fear of gaining weight and a distorted body image.
Choice D reason: Recognizing a codependent relationship and the enabling of unhealthy behaviors shows an understanding of the dynamics that can contribute to the maintenance of an eating disorder like anorexia nervosa.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: Risperidone is an antipsychotic medication commonly used to treat positive symptoms of schizophrenia, such as hallucinations or delusions.
Choice B reason: Haloperidol can be used to treat positive symptoms, but it is not as commonly used as risperidone due to its side effect profile.
Choice C reason: Clonazepam is typically used for anxiety or seizure disorders and is not the primary medication for treating schizophrenia symptoms.
Choice D reason: Clozapine is often reserved for treatment-resistant schizophrenia and is used to treat both positive and negative symptoms, but it is not the first-line treatment due to its potential side effects.
Correct Answer is D
Explanation
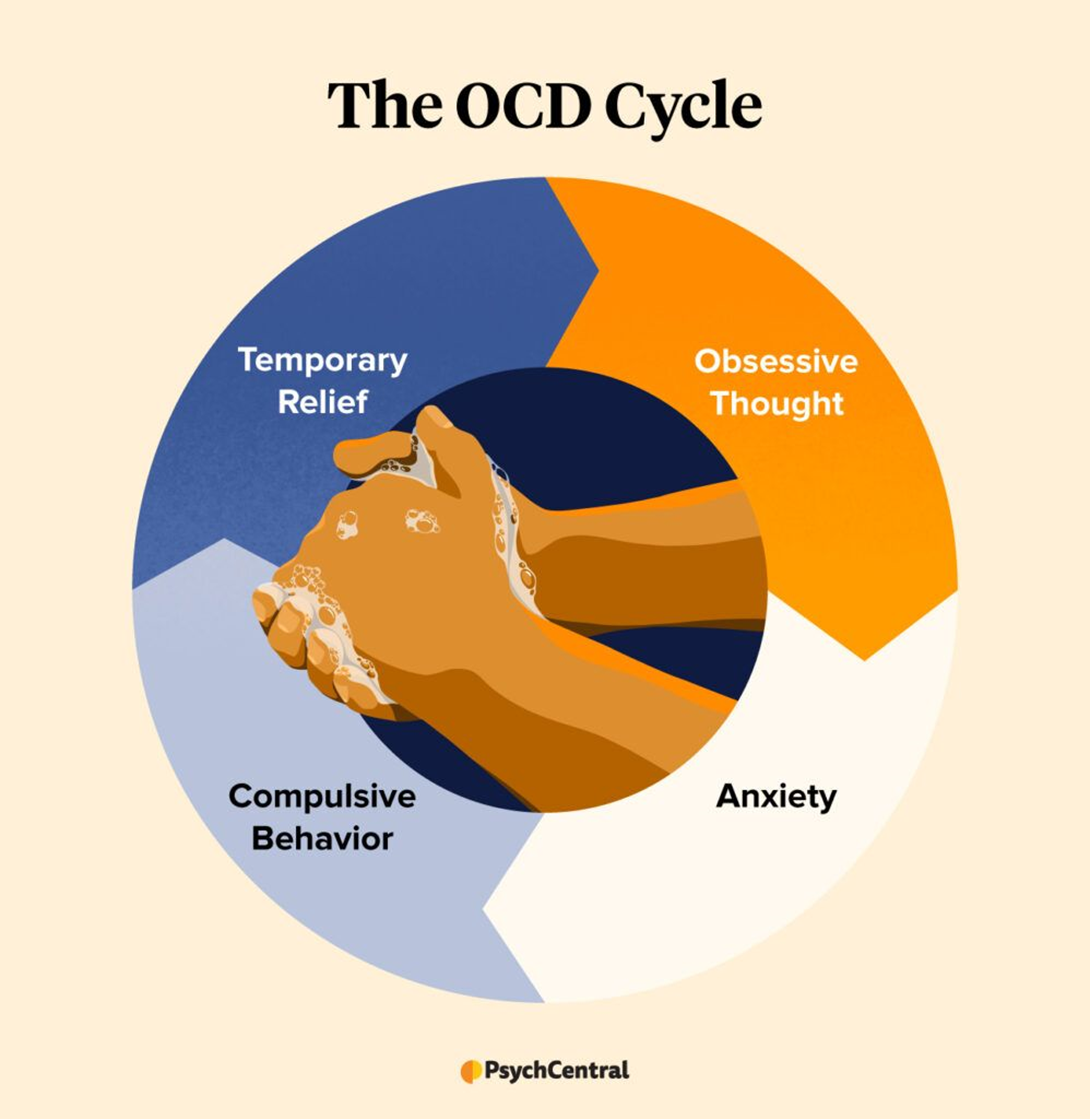
Choice A reason: OCD behaviors are not typically aimed at preventing aggressive and impulsive behaviors but are a response to anxiety-provoking obsessions.
Choice B reason: The repetitive behaviors associated with OCD, such as cleaning, are not intended to manipulate others but are compulsions that the individual feels driven to perform.
Choice C reason: The goal of repetitive cleaning in OCD is not to decrease social interaction time but to alleviate the distress caused by obsessive thoughts, often related to cleanliness or contamination.
Choice D reason: Repetitive cleaning in OCD is a compulsion that aims to decrease the anxiety caused by obsessive thoughts. It is a way for the individual to manage their anxiety and gain a sense of control over their environment.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today