A nurse is collecting data from a client who has placenta previa. Which of the following findings should the nurse expect?
Bright red vaginal bleeding
Rigid abdomen
Increased fetal movement
Persistent uterine contractions
The Correct Answer is A
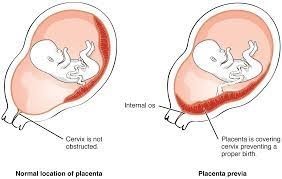
Placenta previa is a condition where the placenta partially or completely covers the cervix, leading to vaginal bleeding. The bleeding is typically painless and bright red in color. This is an important finding that should be assessed and monitored closely.
A rigid abdomen is not a characteristic finding of placenta previa. It could be a sign of another condition such as placental abruption or uterine rupture, which are separate complications. Fetal movement is not directly related to placenta previa. It is a normal finding and can vary depending on the gestational age and individual fetal patterns.
Placenta previa is not typically associated with persistent uterine contractions. However, it is important to monitor for any signs of preterm labor or other complications that could cause uterine contractions.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Wearing a medical identification wristband is important for children with chronic conditions such as cystic fibrosis. It helps alert others, including healthcare providers, about the child's condition in case of emergencies. The wristband can provide vital information about the child's diagnosis, treatment needs, and emergency contacts, ensuring appropriate care and timely interventions.
The other options mentioned are not appropriate or necessary for the care of a child with cystic fibrosis:
A- It is important to involve the child to an age-appropriate extent in decision-making about their treatment. Encouraging the child to participate in their own care and treatment decisions can promote their independence and self-management skills.
B- The influenza vaccine is generally recommended for children with cystic fibrosis, as they are at increased risk of respiratory infections. The vaccine helps protect against influenza and its potential complications. Therefore, the nurse should emphasize the importance of annual influenza vaccination for the child.
D- Homeschooling may not be necessary solely based on the diagnosis of cystic fibrosis. The decision regarding the child's education should be made based on their individual needs, abilities, and preferences, in consultation with the child's healthcare team and educational professionals.
Correct Answer is ["A","B","C","E","G"]
Explanation
Based on the given information, the nurse should take the following actions in preparation for surgery:
- Obtain a complete blood count: This is important to assess the client's hemoglobin, hematocrit, and other blood parameters before surgery.
- Prepare the client for insertion of an 18-gauge peripheral IV prior to surgery: Adequate IV access is necessary for the administration of fluids and medications during and after surgery.
- Administer Rh, D immune globulin prior to surgery: This action is indicated if the client is Rh-negative and there is a possibility of fetal-maternal blood mixing during the termination of pregnancy. Rh, D immune globulin is given to prevent sensitization to Rh-positive blood.
- Verify consent form is signed by the client: Ensuring that the client has provided informed consent is essential before proceeding with any surgical intervention.
- Remind the client to be NPO (nothing by mouth) prior to surgery: It is important for the client to have an empty stomach to reduce the risk of aspiration during anesthesia.
The following actions are not indicated based on the given information:
- Explaining the surgical procedure to the client: Although it is important for the client to have an understanding of the procedure, this is typically done by the surgeon rather than the nurse.
- Assisting with administration of AB positive blood products if needed: There is no indication of the need for blood products based on the information provided. Blood product administration would be determined based on the client's specific condition and surgical requirements.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today