A nurse is collecting data from a client who has heart failure. The nurse notes the client has crackles in the bases of the lungs and a respiratory rate of 24/min. Which of the following actions should the nurse take?
Increase the client's intake of oral fluids.
Instruct the client to cough every 4 hr.
Encourage the client to ambulate to loosen secretions.
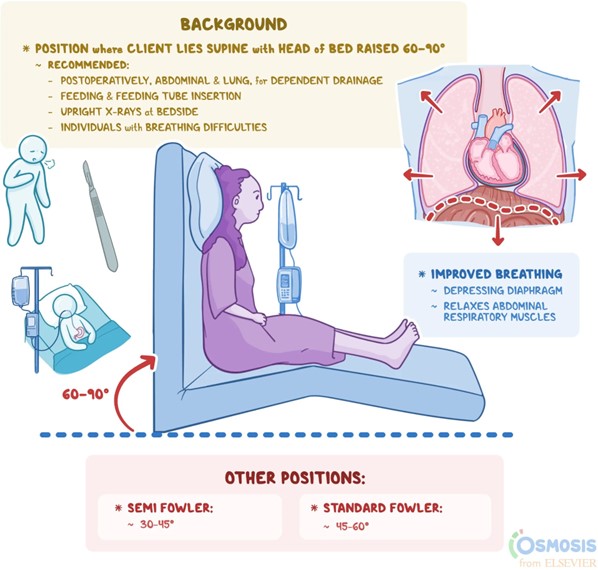
Maintain the client in high-Fowler's position.
The Correct Answer is D
The client's crackles in the bases of the lungs and an increased respiratory rate indicate the presence of fluid accumulation in the lungs, which is commonly seen in clients with heart failure. Maintaining the client in a high Fowler's position helps to promote optimal lung expansion and ventilation by reducing the pressure on the diaphragm, allowing for improved breathing mechanics and enhanced oxygenation.
Increasing the client's intake of oral fluids: While maintaining hydration is generally important, increasing oral fluids may not directly address the issue of fluid accumulation in the lungs. The priority in this situation is to optimize the client's respiratory function.
Instructing the client to cough every 4 hours: Coughing alone may not be sufficient to resolve the fluid accumulation. The underlying cause of the crackles and increased respiratory rate in heart failure is fluid congestion, which requires more comprehensive management.
Encouraging the client to ambulate to loosen secretions: While ambulation is generally beneficial for clients with heart failure, it may not directly address the fluid accumulation in the lungs. Ambulation can help improve overall cardiovascular function and fluid balance, but in the presence of acute respiratory distress or significant fluid overload, the client may not be able to tolerate or benefit from ambulation immediately.
In addition to maintaining the client in a high-Fowler's position, the nurse should also collaborate with the healthcare provider to initiate appropriate interventions, such as administering diuretic medications to help remove excess fluid and improve respiratory status. Monitoring the client's oxygen saturation, providing supplemental oxygen as needed, and assessing other vital signs are also important aspects of care in managing heart failure-related respiratory symptoms.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
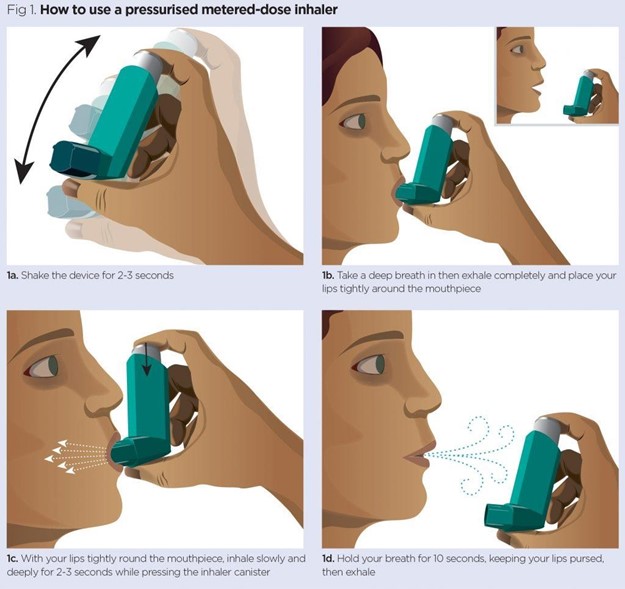
Closing the mouth around the mouthpiece ensures that the medication is delivered directly into the airways. It helps to create a seal and prevents the medication from escaping through the sides of the mouth. This allows for effective delivery of the medication to the lungs.
Option A, exhaling immediately after inhaling, is not correct. The client should inhale slowly and deeply through the mouth, hold their breath for a few seconds, and then exhale slowly. This allows the medication to reach the lungs and be absorbed effectively.
Option C, tilting the head forward while inhaling, is not necessary for using an inhaler. The client should maintain an upright position to ensure proper inhalation and prevent the medication from going down the throat.
Option D, taking three quick breaths while depressing the canister, is not correct. The client should take one slow and deep breath while depressing the canister to release a single dose of medication. This allows the medication to be properly delivered and inhaled into the lungs.
Correct Answer is C
Explanation
Phenytoin is known to cause gingival hyperplasia, which is characterized by swollen and enlarged gums. This side effect is more common in long-term use and may require dental care and regular oral hygiene practices.
Phenytoin is known to be associated with an increased risk of birth defects in babies born to women taking the medication during pregnancy. It is important for women of childbearing age to discuss the risks and benefits of phenytoin with their healthcare provider and use effective contraception to avoid pregnancy while taking the medication.
Phenytoin can affect liver function, so regular monitoring of liver enzymes and blood levels of the medication is necessary. The frequency of blood work may vary depending on the individual's specific situation, so it is important to follow the healthcare provider's instructions.
It is not advisable to skip a dose of phenytoin without consulting a healthcare provider. Abruptly stopping or missing doses of antiepileptic medications can lead to breakthrough seizures or other complications. Any changes in the medication regimen should be discussed with the healthcare provider.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today