A nurse is caring for a client who had an evacuation of a subdural hematoma. Which of the following actions should the nurse take first?
Observe for cerebrospinal fluid (CSF) leaks from the evacuation site.
Check the oximeter.
Assess for an increase in temperature.
Monitor for manifestations of increased intracranial pressure.
The Correct Answer is B
Choice A Reason: Observing for cerebrospinal fluid (CSF) leaks from the evacuation site is important, but not the first action that the nurse should take. CSF leaks can indicate a breach in the dura mater, which can increase the risk of infection and meningitis. The nurse should inspect the dressing and the nose and ears for any clear or bloody drainage, and report any findings to the provider. However, these measures are secondary to ensuring adequate oxygenation and perfusion.
Choice B Reason: The first action the nurse should take when caring for a client post-evacuation of a subdural hematoma is to check the oximeter to ensure adequate oxygenation. Maintaining proper oxygenation is a priority because hypoxia and hypercapnia can lead to cerebral vasodilation, increasing intracranial pressure (ICP) and worsening neurological outcomes. Key Concept: Always prioritize Airway, Breathing, and Circulation (ABCs) when determining the most immediate nursing intervention.
Choice C Reason: Assessing for an increase in temperature is another important action, but not the first one that the nurse should take. An increase in temperature can indicate an infection, inflammation, or damage to the hypothalamus, which can affect the thermoregulation of the body. The nurse should monitor the temperature and administer antipyretics as prescribed. However, these measures are secondary to ensuring adequate oxygenation and perfusion.
Choice D Reason:This is crucial, but oxygenation status should be checked first since low oxygen levels can worsen ICP.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A: Eliciting the gag reflex is a way to assess cranial nerve IX (glossopharyngeal) and X (vagus), which are responsible for the sensation and motor function of the pharynx and larynx.
Choice B: Testing visual acuity is a way to assess cranial nerve II (optic), which is responsible for the sense of vision.
Choice C: Observing for facial symmetry is a way to assess cranial nerve VII (facial), which is responsible for the motor function of the facial muscles and the sensation of taste.
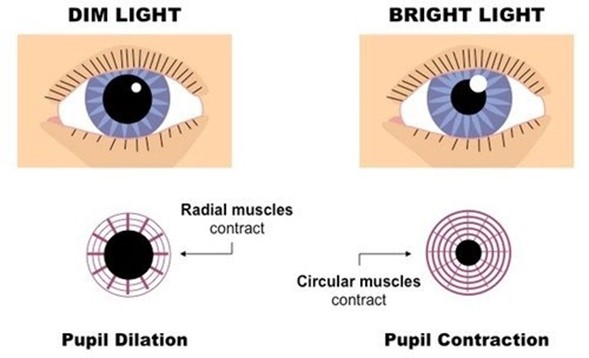
Choice D: Checking the pupillary response to light is a way to assess cranial nerve III (oculomotor), which is responsible for the motor function of most of the eye muscles, including those that control pupil size and lens shape.
Correct Answer is D
Explanation
Choice A Reason: This is incorrect because crepitus in the area above and surrounding the insertion site is not a serious finding that requires notification of the provider. Crepitus is a crackling sensation that occurs when air leaks into the subcutaneous tissue. It is usually harmless and resolves on its own.
Choice B reason: This is incorrect because bubbling of the water in the water seal chamber with exhalation is a normal finding that indicates that air is being removed from the pleural space. Bubbling should stop when the pneumothorax is resolved.
Choice C Reason: This is incorrect because eyelets are not visible is not a serious finding that requires notification of the provider. Eyelets are small holes at the end of the chest tube that allow air and fluid to drain from the pleural space. They are usually covered by a dressing and may not be visible.
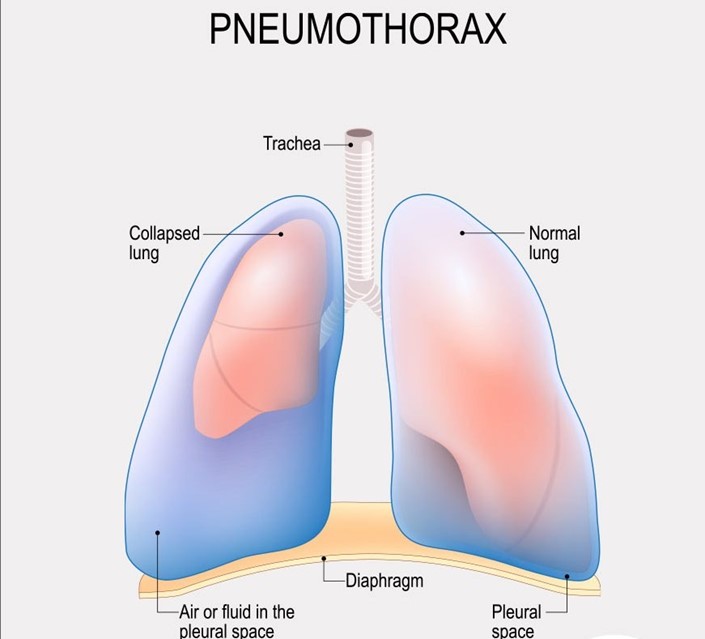
Choice D Reason: This is correct because movement of the trachea toward the unaffected side is a serious finding that indicates a tension pneumothorax, which is a life-threatening condition that occurs when air accumulates in the pleural space and causes pressure on the mediastinum. The nurse should notify the provider immediately and prepare for needle decompression or chest tube insertion.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today