The nurse is caring for a postoperative client who has a chest tube connected to suction and a water seal drainage system. Which of the following indicates to the nurse that the chest tube is functioning properly?
Equal amount of fluid drainage in each collection chamber
Fluctuation of the fluid level within the water seal chamber
Continuous bubbling within the water seal chamber
Absence of fluid in the drainage tubing
The Correct Answer is B
Choice A Reason: Equal amount of fluid drainage in each collection chamber is not a sign of proper chest tube function. The amount of fluid drainage depends on the type and extent of the client's injury or surgery, and may vary from one chamber to another.
Choice B Reason: Fluctuation of the fluid level in the water seal chamber (tidaling) indicates that the chest tube is functioning properly. This fluctuation corresponds with the client's respirations and shows that air or fluid is being effectively removed from the pleural space.
Choice C Reason:Continuous bubbling within the water seal chamber: Continuous bubbling in the water seal chamber indicates an air leak, which is not normal unless the client has a pneumothorax and air is being evacuated. Otherwise, it suggests a problem with the system.
Choice D Reason: Absence of fluid in the drainage tubing is not a sign of proper chest tube function. It may indicate that the chest tube is obstructed, kinked, or clamped, or that the suction is not working properly. The nurse should assess and troubleshoot the chest tube system.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: This choice is incorrect because slowing the rate to 50 mL/hr may not be enough to prevent cerebral edema, which is a common complication of head injury. Cerebral edema is a swelling of the brain tissue due to increased fluid accumulation. It can cause increased intracranial pressure (ICP), which can lead to brain damage or death. Therefore, the nurse should limit the fluid intake of the client with head injury to avoid worsening the condition.
Choice B Reason: This choice is incorrect because increasing the rate to 250 mL/hr may cause fluid overload, which can also increase the ICP and worsen the cerebral edema. Fluid overload is a condition in which the body has too much fluid, which can impair the function of the heart, lungs, and kidneys. Therefore, the nurse should avoid giving too much fluid to the client with head injury.
Choice C reason: Reducing the infusion to 20 mL/hr is excessively low and may cause hypotension or inadequate maintenance of vascular access and medication delivery. Such a drastic decrease could impair perfusion to injured brain tissue and is not an appropriate independent nursing action without a specific order.
Choice D reason: Maintaining the current prescribed infusion rate avoids abrupt volume shifts that could alter intracranial pressure. The nurse should monitor neurologic status and vital signs, ensure the IV is patent, and follow provider orders; only change the rate when clinically indicated or when directed by the prescriber.
Correct Answer is D
Explanation
Choice A: Eliciting the gag reflex is a way to assess cranial nerve IX (glossopharyngeal) and X (vagus), which are responsible for the sensation and motor function of the pharynx and larynx.
Choice B: Testing visual acuity is a way to assess cranial nerve II (optic), which is responsible for the sense of vision.
Choice C: Observing for facial symmetry is a way to assess cranial nerve VII (facial), which is responsible for the motor function of the facial muscles and the sensation of taste.
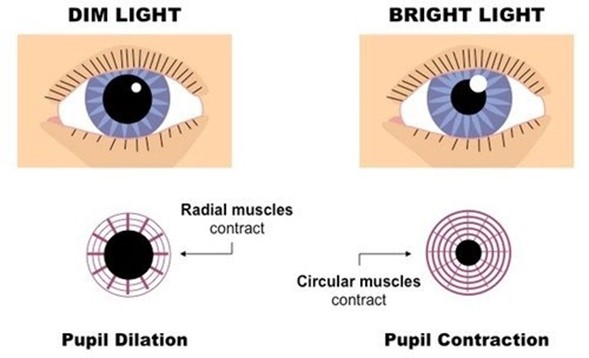
Choice D: Checking the pupillary response to light is a way to assess cranial nerve III (oculomotor), which is responsible for the motor function of most of the eye muscles, including those that control pupil size and lens shape.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today