A nurse is monitoring the pulmonary artery wedge pressure (PAWP) for a client. The nurse should identify that a reading of 17 mm Hg is an indication of which of the following conditions?
Right ventricular failure
Fluid volume deficit
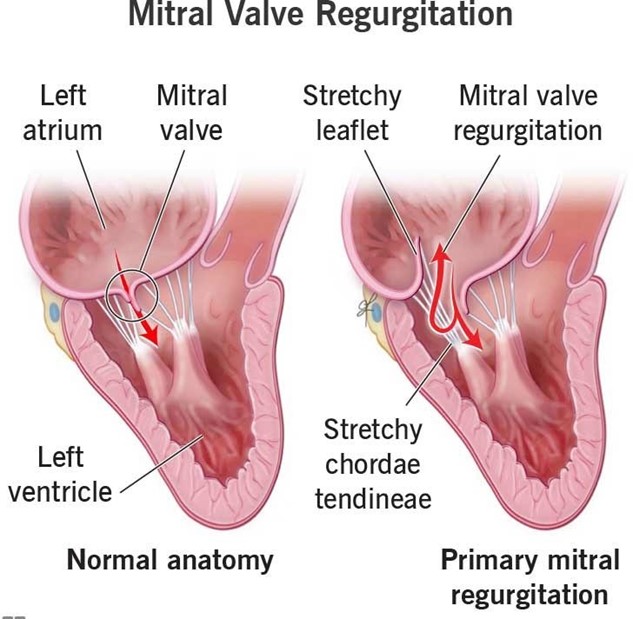
Mitral regurgitation
Afterload reduction
The Correct Answer is C
Choice A Reason: This is incorrect because right ventricular failure would cause an increase in right atrial pressure and right ventricular end-diastolic pressure, but not in PAWP, which reflects left atrial pressure and left ventricular end- diastolic pressure.
Choice B Reason: This is incorrect because fluid volume deficit would cause a decrease in PAWP, as there would be less blood volume in the pulmonary circulation.
Choice C Reason: This is correct because mitral regurgitation would cause an increase in PAWP, as the blood would back up into the left atrium and pulmonary veins due to the incompetent mitral valve.
Choice D Reason: This is incorrect because afterload reduction would cause a decrease in PAWP, as there would be less resistance to the left ventricular ejection and less blood volume in the pulmonary circulation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: This choice is incorrect because it indicates respiratory alkalosis, not AKI. Respiratory alkalosis is a condition in which the lungs eliminate too much carbon dioxide (CO2) from the blood, resulting in a low level of CO2 (PaCO2) and a high level of pH. A normal PaCO2 range is 35 to 45 mm Hg, and a normal pH range is 7.35 to 7.45, so a value of 30 mm Hg and 7.49 indicate respiratory alkalosis.
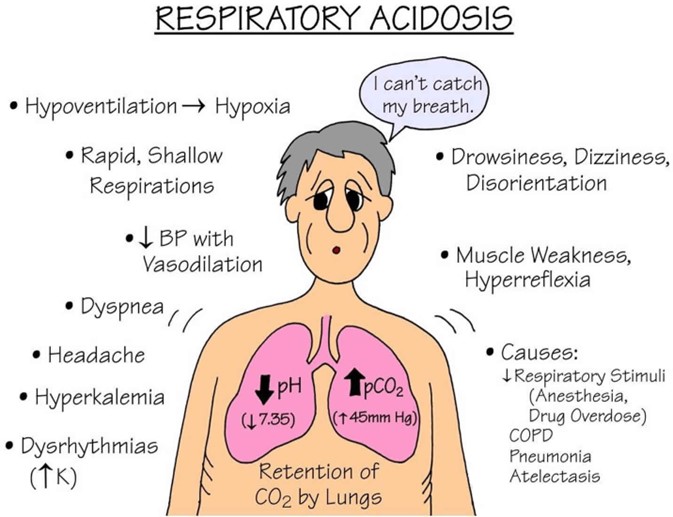
Choice B Reason: This choice is incorrect because it indicates respiratory acidosis, not AKI. Respiratory acidosis is a condition in which the lungs cannot eliminate enough CO2 from the blood, resulting in a high level of CO2 (PaCO2) and a low level of pH. A value of 46 mm Hg and 7.26 indicate respiratory acidosis.
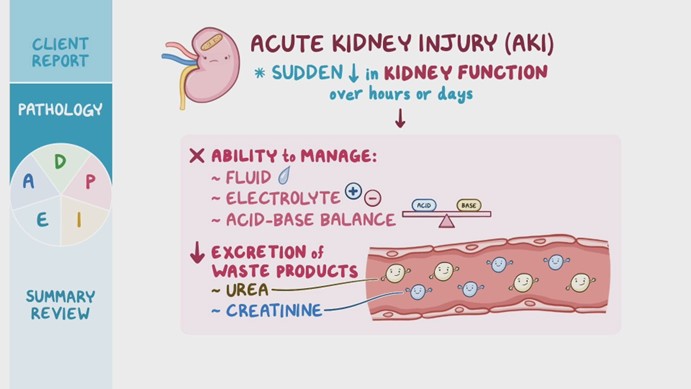
Choice C Reason: This choice is correct because it indicates metabolic acidosis, which is a common complication of AKI. Metabolic acidosis is a condition in which the body produces too much acid or loses too much base, resulting in a low level of bicarbonate (HCO3) and a low level of pH. A normal HCO3 range is 22 to 26 mEq/L, so a value of 14 mEq/L indicates metabolic acidosis. The low PaCO2 value (30 mm Hg) is due to the respiratory compensation mechanism that tries to restore the acid-base balance by increasing the ventilation and eliminating more CO2.
Choice D Reason: This choice is incorrect because it indicates metabolic alkalosis, not AKI. Metabolic alkalosis is a condition in which the body loses too much acid or gains too much base, resulting in a high level of bicarbonate (HCO3) and a high level of pH. A value of 30 mEq/L and 7.49 indicate metabolic alkalosis.
Correct Answer is A
Explanation
Choice A Reason: This choice is correct because respiratory acidosis is a condition in which the lungs cannot eliminate enough carbon dioxide (CO2) from the blood, resulting in a high level of CO2 (PaCO2) and a low level of pH. A normal PaCO2 range is 35 to 45 mm Hg, so a value of 50 mm Hg indicates respiratory acidosis.
Choice B Reason: This choice is incorrect because HCO3 (bicarbonate) is a base that helps to buffer the excess acid in the blood. In respiratory acidosis, the kidneys try to compensate by retaining more HCO3 and excreting more hydrogen ions. Therefore, a high level of HCO3 (above 26 mEq/L) would indicate a chronic or compensated respiratory acidosis, not an acute or uncompensated one.
Choice C Reason: This choice is incorrect because pH is a measure of the acidity or alkalinity of the blood. A normal pH range is 7.35 to 7.45, so a value of 7.45 indicates a neutral or slightly alkaline blood, not an acidic one. A low pH (below 7.35) would indicate respiratory acidosis.
Choice D Reason: This choice is incorrect because potassium is an electrolyte that helps to regulate the nerve and muscle function, as well as the fluid balance in the body. In respiratory acidosis, the increased hydrogen ions in the blood may shift into the cells in exchange for potassium, resulting in a high level of potassium (hyperkalemia).
Therefore, a low level of potassium (below 3.5 mEq/L) would indicate hypokalemia, not respiratory acidosis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today