A nurse is reviewing the PT, aPTT, and INR laboratory values for a client who is experiencing an acute episode of disseminated intravascular coagulation (DIC). Which of the following laboratory results should the nurse expect?
The laboratory values are within the expected reference range.
The laboratory values are prolonged.
The laboratory values are the same as the previous test values.
The laboratory values are decreased.
The Correct Answer is B
Choice A Reason: This is incorrect because the laboratory values are not within the expected reference range in a client who has DIC. DIC is a condition that causes abnormal activation of the clotting cascade, leading to widespread microthrombi formation and consumption of clotting factors and platelets. This results in bleeding complications and organ dysfunction.
Choice B Reason: This is correct because the laboratory values are prolonged in a client who has DIC. PT, aPTT, and INR are tests that measure the time it takes for blood to clot. PT measures the extrinsic pathway, aPTT measures the intrinsic pathway, and INR is a standardized ratio of PT. In DIC, these tests are prolonged because of the depletion of clotting factors and platelets.
Choice C Reason: This is incorrect because the laboratory values are not the same as the previous test values in a client who has DIC. DIC is an acute and dynamic condition that can change rapidly depending on the underlying cause and treatment. The laboratory values may fluctuate between normal, prolonged, or shortened depending on the balance between clotting and bleeding.
Choice D Reason: This is incorrect because the laboratory values are not decreased in a client who has DIC. Decreased laboratory values would indicate a shortened clotting time, which can occur in some cases of DIC when there is excessive clotting and thrombosis. However, this is not the typical finding in DIC, as most clients present with bleeding manifestations and prolonged clotting time.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["24"]
Explanation
- To find the concentration of heparin in the solution, divide the amount of heparin by the volume of D5W: 25,000 units / 500 mL = 50 units/mL
- To find the infusion rate, divide the prescribed dose by the concentration: 1,200 units/hr / 50 units/mL = 24 mL/hr
- Round the answer to the nearest tenth/whole number: 24 mL/hr
Correct Answer is D
Explanation
Choice A Reason: This is incorrect because crepitus in the area above and surrounding the insertion site is not a serious finding that requires notification of the provider. Crepitus is a crackling sensation that occurs when air leaks into the subcutaneous tissue. It is usually harmless and resolves on its own.
Choice B reason: This is incorrect because bubbling of the water in the water seal chamber with exhalation is a normal finding that indicates that air is being removed from the pleural space. Bubbling should stop when the pneumothorax is resolved.
Choice C Reason: This is incorrect because eyelets are not visible is not a serious finding that requires notification of the provider. Eyelets are small holes at the end of the chest tube that allow air and fluid to drain from the pleural space. They are usually covered by a dressing and may not be visible.
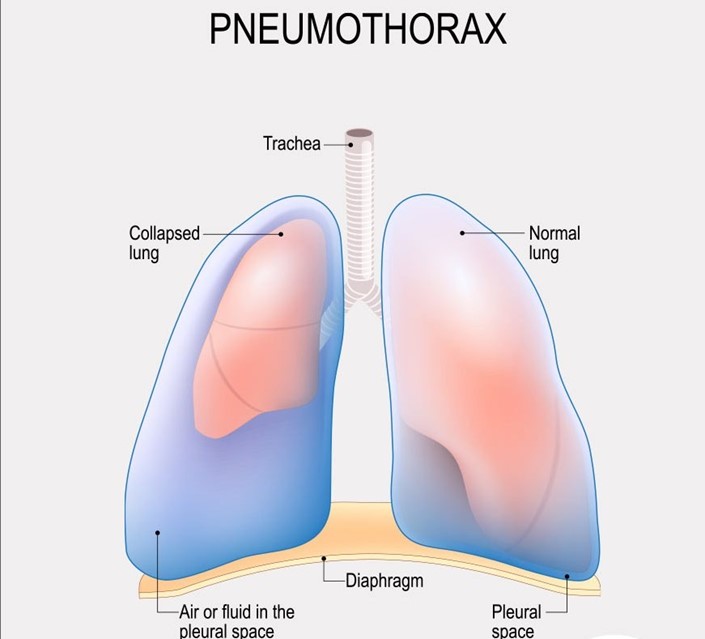
Choice D Reason: This is correct because movement of the trachea toward the unaffected side is a serious finding that indicates a tension pneumothorax, which is a life-threatening condition that occurs when air accumulates in the pleural space and causes pressure on the mediastinum. The nurse should notify the provider immediately and prepare for needle decompression or chest tube insertion.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today