A nurse in the emergency department is caring for a client who has extensive partial and full-thickness burns of the head, neck, and chest. While planning the client's care, the nurse should identify which of the following risks as the priority for assessment and intervention?
Infection
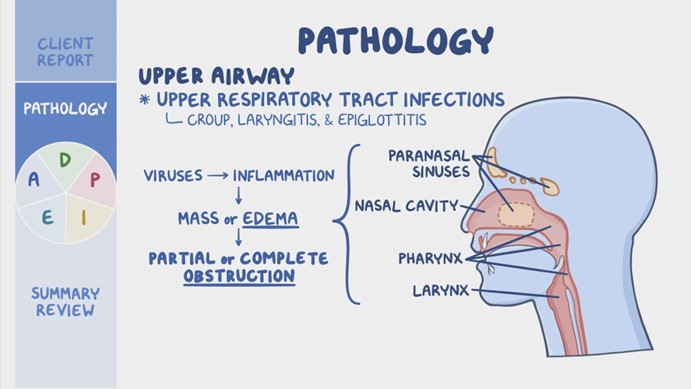
Airway obstruction
Paralytic ileus
Fluid imbalance
The Correct Answer is B
Choice A Reason: Infection is a serious complication of burn injuries, but not the priority risk for assessment and intervention. The nurse should monitor the client's wound healing, temperature, white blood cell count, and signs of sepsis, and administer antibiotics as prescribed. However, these measures are secondary to ensuring adequate oxygenation and ventilation.
Choice B Reason: Airway obstruction is the priority risk for assessment and intervention for a client who has burns of the head, neck, and chest. The nurse should assess the client's airway patency, respiratory rate, oxygen saturation, breath sounds, and signs of respiratory distress, such as stridor, wheezes, or cyanosis. The nurse should also provide humidified oxygen, suction secretions, elevate the head of the bed, and prepare for endotracheal intubation if needed. Airway obstruction can occur due to edema, inflammation, or inhalation injury of the upper airway, and can quickly lead to hypoxia, respiratory failure, and death.
Choice C Reason: Paralytic ileus is a potential complication of burn injuries, but not the priority risk for assessment and intervention. The nurse should assess the client's bowel sounds, abdominal distension, nausea, vomiting, and stool output, and administer fluids, electrolytes, and nutritional support as prescribed. However, these measures are secondary to ensuring adequate oxygenation and ventilation.
Choice D Reason: Fluid imbalance is another potential complication of burn injuries, but not the priority risk for assessment and intervention. The nurse should assess the client's fluid status, urine output, vital signs, weight, and serum electrolytes, and administer intravenous fluids as prescribed. However, these measures are secondary to ensuring adequate oxygenation and ventilation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: This choice is incorrect because urinary hesitancy is not the priority finding for the nurse to address.
Urinary hesitancy is a difficulty or delay in starting or maintaining a urine stream. It may be caused by various factors such as prostate enlargement, urinary tract infection, medication side effects, or psychological issues. It may cause discomfort, pain, or urinary retention, but it does not pose an immediate threat to the client's life.
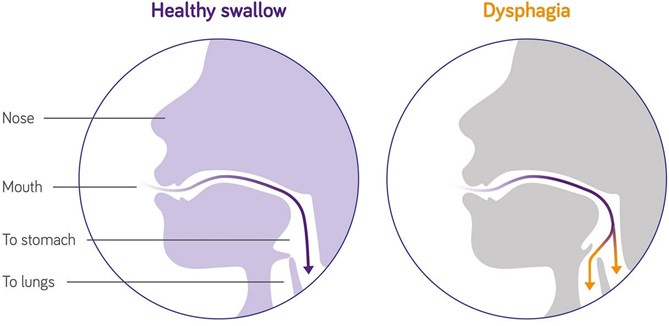
ChoiceB Reason: This choice is correct because dysphagia is the priority finding for the nurse to address. Dysphagia is a difficulty or inability to swallow food or liquids. It may be caused by various factors such as stroke, Parkinson's disease, dementia, esophageal cancer, or oral infections. It may cause malnutrition, dehydration, aspiration, or choking, which can lead to serious complications such as pneumonia, sepsis, or death. Therefore, the nurse should assess the client's swallowing function and provide appropriate interventions such as modifying the diet texture, using thickening agents, or teaching swallowing techniques.
ChoiceC Reason: This choice is incorrect because swollen gums are not the priority finding for the nurse to address. Swollen gums are an inflammation or enlargement of the gingival tissue that surrounds the teeth. They may be caused by various factors such as poor oral hygiene, gum disease, vitamin deficiency, medication side effects, or hormonal changes. They may cause bleeding, pain, or infection, but they do not pose an immediate threat to the client's life.
Choice D Reason: This choice is incorrect because pruritus is not the priority finding for the nurse to address. Pruritus is a sensation of itching that affects the skin. It may be caused by various factors such as dry skin, allergies, eczema, psoriasis, liver disease, or kidney disease. It may cause discomfort, scratching, or skin damage, but it does not pose an immediate threat to the client's life.
Correct Answer is A
Explanation
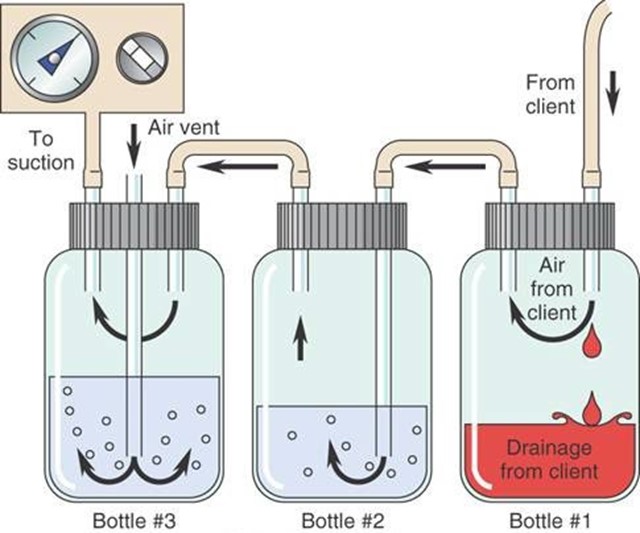
Choice A Reason: Continuous bubbling in the water-seal chamber indicates an air leak in the chest tube system, which can compromise the drainage of air and fluid from the pleural space and impair lung expansion.
Choice B Reason: Occasional bubbling in the water-seal chamber is normal and expected, as it indicates that air is being removed from the pleural space.
Choice C Reason: Fluctuations in the fluid level in the water-seal chamber are normal and expected, as they reflect changes in intrathoracic pressure during inspiration and expiration.
Choice D Reason: Constant bubbling in the suction-control chamber is normal and expected, as it indicates that suction is being applied to the chest tube system.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today