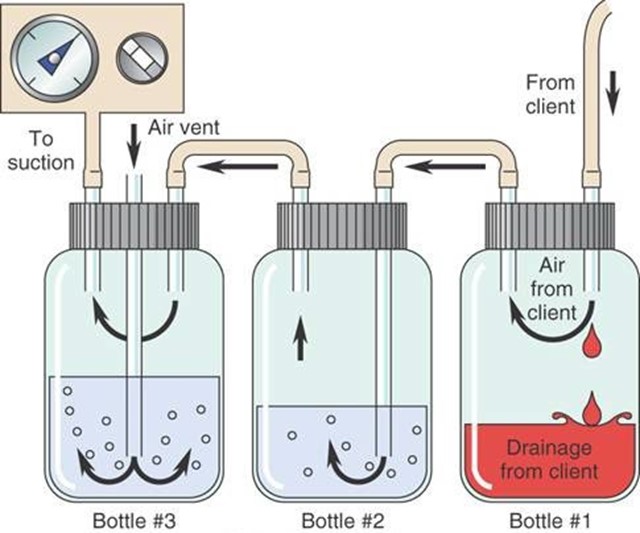
A nurse is caring for a client who has a disposable three-chamber chest tube in place. Which of the following findings should indicate to the nurse that the client is experiencing a complication?
Continuous bubbling in the water-seal chamber
Occasional bubbling in the water-seal chamber
Fluctuations in the fluid level in the water-seal chamber
Constant bubbling in the suction-control chamber
The Correct Answer is A
Choice A Reason: Continuous bubbling in the water-seal chamber indicates an air leak in the chest tube system, which can compromise the drainage of air and fluid from the pleural space and impair lung expansion.
Choice B Reason: Occasional bubbling in the water-seal chamber is normal and expected, as it indicates that air is being removed from the pleural space.
Choice C Reason: Fluctuations in the fluid level in the water-seal chamber are normal and expected, as they reflect changes in intrathoracic pressure during inspiration and expiration.
Choice D Reason: Constant bubbling in the suction-control chamber is normal and expected, as it indicates that suction is being applied to the chest tube system.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: This is incorrect because cognitive impairment that decreases over several months post-injury is more likely to occur in a client who has a diffuse axonal injury, which is a widespread damage to the brain's white mater.
Choice B Reason: This is incorrect because neurologic deficits that increase up to 2 weeks post-injury are more likely to occur in a client who has a subdural hematoma, which is a collection of blood between the dura and the arachnoid membranes.
Choice C Reason: This is incorrect because a change in the level of consciousness that develops over 48 hr is more likely to occur in a client who has an intracerebral hematoma, which is a collection of blood within the brain tissue.
Choice D Reason: This is correct because a lucid period followed by an immediate loss of consciousness is a typical manifestation of an epidural hematoma, which is a collection of blood between the skull and the dura. The lucid period occurs when the initial bleeding stops and the client regains consciousness. The immediate loss of consciousness occurs when the bleeding resumes and causes increased intracranial pressure.
Correct Answer is D
Explanation
Choice A Reason: This is incorrect because administering a nitrate antihypertensive is not the first action, as it may cause a rapid drop in blood pressure and worsen the client's condition.
Choice B Reason: This is incorrect because obtaining the client's heart rate is not the first action, as it does not address the cause of autonomic dysreflexia or relieve the symptoms.
Choice C Reason: This is incorrect because assessing the client for bladder distention is not the first action, as it may take time and delay the treatment of autonomic dysreflexia.
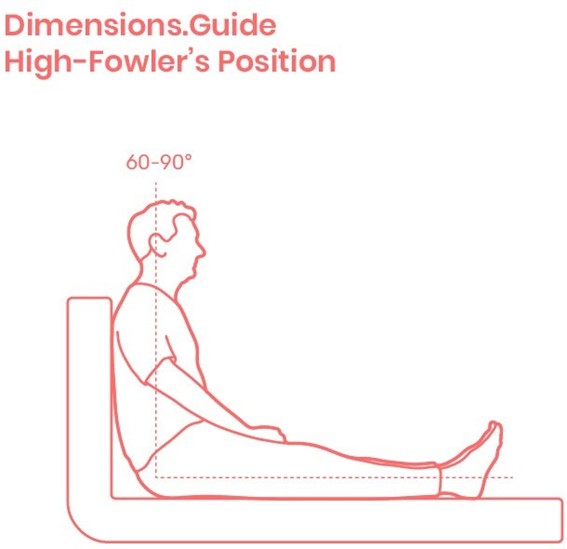
Choice D Reason: This is correct because placing the client in a high-Fowler's position is the first action, as it lowers the blood pressure by promoting venous return and reducing cardiac preload.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today