A nurse is assessing a client's cranial nerves as part of a neurological examination. Which of the following actions should the nurse take to assess cranial nerve III?
Eliciting the gag reflex
Testing visual acuity
Observing for facial symmetry
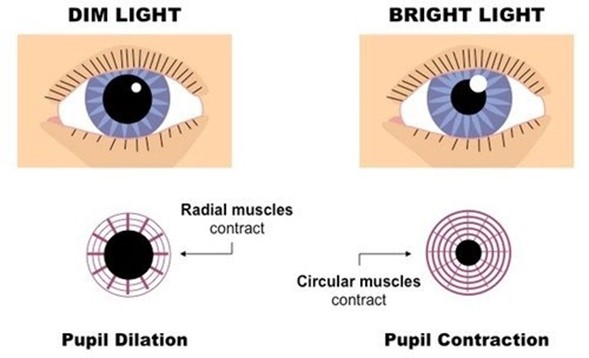
Checking the pupillary response to light
The Correct Answer is D
Choice A: Eliciting the gag reflex is a way to assess cranial nerve IX (glossopharyngeal) and X (vagus), which are responsible for the sensation and motor function of the pharynx and larynx.
Choice B: Testing visual acuity is a way to assess cranial nerve II (optic), which is responsible for the sense of vision.
Choice C: Observing for facial symmetry is a way to assess cranial nerve VII (facial), which is responsible for the motor function of the facial muscles and the sensation of taste.
Choice D: Checking the pupillary response to light is a way to assess cranial nerve III (oculomotor), which is responsible for the motor function of most of the eye muscles, including those that control pupil size and lens shape.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: This choice is incorrect because oral hypoglycemic medications are not effective for treating DKA. Oral hypoglycemic medications are drugs that lower the blood glucose level by stimulating insulin secretion or increasing insulin sensitivity. They may be used for clients who have type 2 diabetes mellitus, but they do not work for clients who have type 1 diabetes mellitus or DKA.
Choice B Reason: This choice is correct because 0.9% sodium chloride IV bolus is an effective treatment for DKA. 0.9% sodium chloride is an isotonic solution that contains the same concentration of solutes as blood plasma. It may be used for clients who have fluid loss, dehydration, or shock. In DKA, the body breaks down fat for energy due to insulin deficiency or resistance, resulting in high levels of ketones and acids in the blood. This causes osmotic diuresis, dehydration, electrolyte imbalance, and metabolic acidosis. Therefore, administering 0.9% sodium chloride IV bolus can help to restore fluid volume and correct electrolyte imbalance.
Choice C Reason: This choice is incorrect because dextrose 5% in 0.45% sodium chloride is not indicated for treating DKA. Dextrose 5% in 0.45% sodium chloride is a hypertonic solution that contains more solutes than blood plasma. It may be used for clients who have hyponatremia, cerebral edema, or malnutrition, but it can worsen hyperglycemia and osmotic diuresis in clients who have DKA.
Choice D Reason: This choice is incorrect because glucocorticoid medications are not indicated for treating DKA. Glucocorticoid medications are drugs that mimic the effects of cortisol, a hormone that regulates stress response and inflammation. They may be used for clients who have allergic reactions, asthma, or autoimmune diseases, but they can increase blood glucose levels and inhibit insulin action in clients who have DKA.
Correct Answer is D
Explanation
Choice A Reason: Dextran 70 is not a medication that the nurse should plan to administer for a client who has a traumatic head injury and is exhibiting signs of increasing intracranial pressure. Dextran 70 is a plasma expander that increases the blood volume and viscosity, which can worsen the intracranial pressure by increasing the cerebral blood flow and edema.
Choice B Reason: Hydroxyethyl starch is not a medication that the nurse should plan to administer for a client who has a traumatic head injury and is exhibiting signs of increasing intracranial pressure. Hydroxyethyl starch is another plasma expander that has similar effects as dextran 70, and can also increase the risk of coagulopathy and renal failure.
Choice C Reason: Albumin 25% is not a medication that the nurse should plan to administer for a client who has a traumatic head injury and is exhibiting signs of increasing intracranial pressure. Albumin 25% is a colloid solution that increases the oncotic pressure and draws fluid from the interstitial space into the intravascular space, which can also worsen the intracranial pressure by increasing the cerebral blood flow and edema.
Choice D Reason: Mannitol 25% is a medication that the nurse should plan to administer for a client who has a traumatic head injury and is exhibiting signs of increasing intracranial pressure. Mannitol 25% is an osmotic diuretic that reduces the intracranial pressure by creating an osmotic gradient and drawing fluid from the brain tissue into the blood vessels, which can then be excreted by the kidneys. The nurse should monitor the urine output, serum osmolality, and electrolytes when administering mannitol 25%.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today