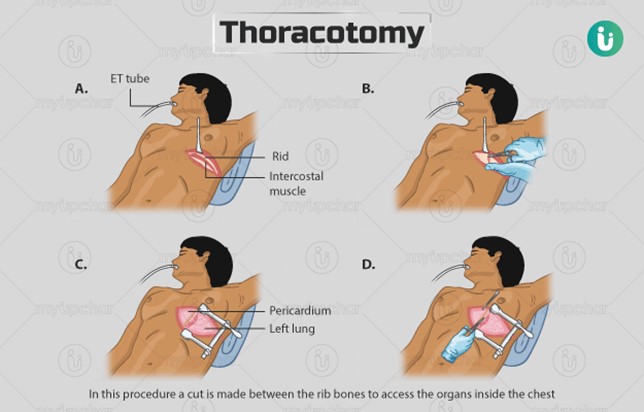
A nurse is observing the closed chest drainage system of a client who is 24 hr post thoracotomy. The nurse notes slow, steady bubbling in the suction control chamber. Which of the following actions should the nurse take?
Continue to monitor the client's respiratory status.
Check the suction control outlet on the wall.
Clamp the chest tube.
Check the tubing connections for leaks.
The Correct Answer is A
Choice A Reason: This choice is correct because slow, steady bubbling in the suction control chamber indicates that the suction is working properly and maintaining a negative pressure in the pleural space. The nurse should continue to monitor the client's respiratory status, such as breath sounds, oxygen saturation, and respiratory rate, to assess the effectiveness of the chest drainage system.
Choice B Reason: This choice is incorrect because checking the suction control outlet on the wall is not necessary unless there is no bubbling in the suction control chamber, which would indicate a problem with the suction source or setting. The nurse should ensure that the suction control outlet is set at the prescribed level, usually between 10 and 20 cm H2O.
Choice C Reason: This choice is incorrect because clamping the chest tube is not indicated unless there is a leak in the system or the chest drainage unit needs to be changed. Clamping the chest tube may cause a buildup of air or fluid in the pleural space, which can lead to tension pneumothorax or pleural effusion.
Choice D Reason: This choice is incorrect because checking the tubing connections for leaks is not necessary unless there is continuous bubbling in the water seal chamber, which would indicate an air leak in the system. The nurse should ensure that all tubing connections are tight and secure, and tape any loose connections.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A Reason: This is correct because an osmotic diuretic, such as mannitol, works by creating an osmotic gradient that draws fluid from the brain tissue into the blood vessels, thereby reducing cerebral edema and intracranial pressure.
Choice B Reason: This is incorrect because an osmotic diuretic would decrease, not increase, the cell size in the brain by removing fluid from the intracellular space.
Choice C Reason: This is incorrect because an osmotic diuretic would decrease, not expand, the extracellular fluid volume by increasing the urine output and excreting excess fluid from the body.
Choice D Reason: This is incorrect because an osmotic diuretic would not provide fluid hydration, but rather cause fluid loss and dehydration.
Correct Answer is C
Explanation
Choice A Reason: This is incorrect because fluid overload is a condition of excess fluid volume in the body. A client who has fluid overload is more likely to have a high CVP, which indicates increased pressure in the right atrium and vena cava.
Choice B Reason: This is incorrect because an intracardiac shunt is a condition of abnormal blood flow between the chambers of the heart. A client who has an intracardiac shunt may have a normal or high CVP, depending on the direction and magnitude of the shunt.
Choice C Reason: This is correct because hypovolemia is a condition of low fluid volume in the body. A client who has hypovolemia is more likely to have a low CVP, which indicates decreased pressure in the right atrium and vena cava.
Choice D Reason: This is incorrect because left ventricular failure is a condition of impaired pumping function of the left ventricle. A client who has left ventricular failure may have a normal or high CVP, depending on the degree of backward failure and pulmonary congestion.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today