Why is it important for the nurse to assess the bladder regularly and encourage the laboring client to void every 2 hours?
Select one:
Frequent voiding encourages sphincter control.
A full bladder impedes oxygen flow to the fetus.
Frequent voiding prevents bruising of the bladder.
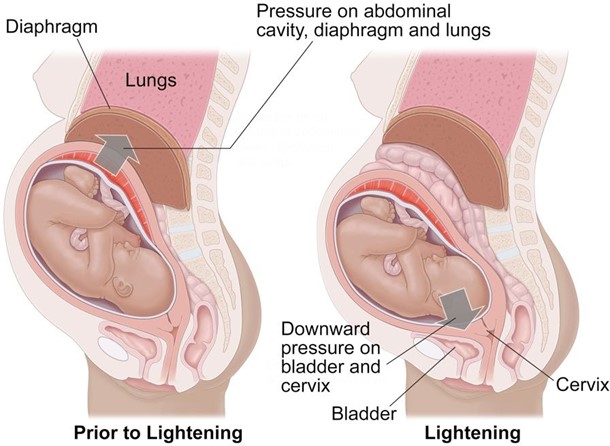
A full bladder can impede fetal descent.
The Correct Answer is D
Choice A Reason: Frequent voiding encourages sphincter control. This is an incorrect statement that has no relevance to labor and delivery. Sphincter control refers to the ability to contract and relax the muscles that control urination and defecation. It is not affected by frequent voiding.
Choice B Reason: A full bladder impedes oxygen flow to the fetus. This is an incorrect statement that confuses a full bladder with a prolapsed cord. A prolapsed cord is a condition where the umbilical cord slips through the cervix before the baby and becomes compressed by the fetal head, which can reduce oxygen flow to the fetus. A full bladder does not affect oxygen flow to the fetus.
Choice C Reason: Frequent voiding prevents bruising of the bladder. This is an incorrect statement that exaggerates the effect of a full bladder on the bladder wall. A full bladder may cause some pressure or discomfort on the bladder, but it does not cause bruising or damage.
Choice D Reason: A full bladder can impede fetal descent. This is a correct statement that explains why it is important for the nurse to assess the bladder regularly and encourage the laboring client to void every 2 hours.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A Reason: Fetal movements are an indicator of fetal well-being. You should count twice a day, and you should feel ten fetal movements in 2 hours. This is because this response provides accurate and clear instructions on how to perform kick counts, which are a simple and non-invasive method of monitoring fetal activity and health. Kick counts can help detect changes in fetal movement paterns that may indicate fetal distress or hypoxia.
Choice B Reason: Here is a computer printed information packet on how to do kick counts. This is an insufficient answer that does not address the patient's question or demonstrate effective communication skills. Providing writen information alone may not ensure the patient's understanding or compliance with kick counts.
Choice C Reason: Fetal kick counts are not a reliable indicator of fetal well-being in the third trimester. This is an incorrect answer that contradicts the evidence and guidelines on kick counts. Kick counts are recommended for all pregnant women, especially in the third trimester, when fetal movements are more noticeable and consistent.
Choice D Reason: It is not important to do kick counts because you have a low-risk pregnancy. This is an incorrect answer that discourages the patient from performing kick counts and may give her a false sense of security. Kick counts are important for all pregnant women, regardless of their risk status, as they can help identify potential problems that may require further evaluation or intervention.
Correct Answer is D
Explanation
Choice A Reason: "Your body is responding to the events of labor, just like after a tough workout." This is an inaccurate statement that does not explain the cause of the contractions or reassure the client.
Choice B Reason: "This could be a sign that your body is trying to get rid of retained placental fragments." This is an alarming statement that may scare the client and imply that something is wrong. Retained placental fragments are rare and usually cause heavy bleeding, fever, and infection.
Choice C Reason: "Let me check your vaginal discharge just to make sure everything is fine." This is an unnecessary statement that does not answer the client's question or provide any information.
Choice D Reason:"The baby's sucking releases oxytocin which causes your uterus to contract." This is a correct statement that explains the physiological mechanism of the contractions and reassures the client that they are normal and beneficial.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today