The nurse's initial action when caring for an otherwise stable, full term infant with a slightly decreased temperature is to:
Select one:
Place the infant skin to skin with the mother and re-check temperature in 30 minutes.
Check the infant's CBC and blood cultures, as this is a sign of probable sepsis.
Return the infant to the nursery for close observation under warming lights.
Notify the physician immediately and suggest orders for placement in an incubator.
The Correct Answer is A
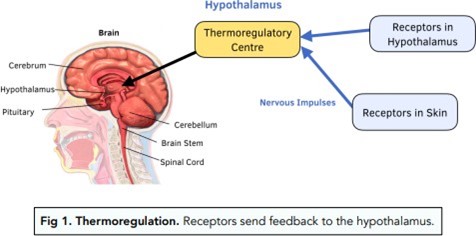
Choice A Reason: Place the infant skin to skin with the mother and re-check temperature in 30 minutes. This is because skin-to-skin contact is an effective and safe method of increasing the infant's temperature and promoting thermoregulation. Skin-to-skin contact also has other benefits such as enhancing bonding, breastfeeding, and maternal-infant attachment.
Choice B Reason: Check the infant's CBC and blood cultures, as this is a sign of probable sepsis. This is an unnecessary action that may cause undue stress and discomfort to the infant and the mother. A slightly decreased temperature in a full-term infant is not a sign of probable sepsis, but rather a common finding that may be due to environmental factors, such as exposure to cold air or wet linens.
Choice C Reason: Return the infant to the nursery for close observation under warming lights. This is an undesirable action that may interfere with the early initiation of breastfeeding and bonding between the mother and the infant. Warming lights are not recommended for routine use in healthy newborns, as they may cause dehydration, hyperthermia, or eye damage.
Choice D Reason: Notify the physician immediately and suggest orders for placement in an incubator. This is an excessive action that may indicate a lack of knowledge or confidence on the part of the nurse. An incubator is not indicated for a stable, full term infant with a slightly decreased temperature, as it may expose the infant to unnecessary interventions, infections, or separation from the mother.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: "My baby will always be smaller than other babies his age." This is an incorrect answer that indicates a misconception or pessimism about SGA newborns. SGA newborns may not always be smaller than other babies their age, as they may catch up in growth and development with appropriate nutrition and care. SGA newborns may have different growth paterns depending on the cause and timing of their growth restriction.
Choice B Reason: "My baby will be okay as long as he has frequent feedings." This is an incorrect answer that indicates an oversimplification or optimism about SGA newborns. SGA newborns may not be okay with just frequent feedings, as they may have other problems or complications that require medical atention and intervention. SGA newborns may have increased nutritional needs and feeding difficulties due to low birth weight, poor suck-swallow coordination, or oral aversion.
Choice C Reason: "My baby will need to stay in the hospital until he weighs 5 pounds." This is an incorrect answer that indicates a misunderstanding or confusion about SGA newborns. SGA newborns may not need to stay in the hospital until they weigh 5 pounds, as they may be discharged earlier or later depending on their condition and readiness for home care. SGA newborns may have different criteria for discharge based on their gestational age, weight gain, feeding tolerance, temperature stability, and absence of complications.
Choice D Reason: "My baby can get cold easily, may have low blood sugar, and may have trouble breathing." This is because this statement by the parents indicates that they understand some of the common problems and complications that SGA newborns may face. SGA newborns are those who weigh less than the 10th percentile for their gestational age, which can be due to intrauterine growth restriction (IUGR) or constitutional factors. SGA newborns may have difficulties with thermoregulation, glucose metabolism, and respiratory function due to inadequate fat stores, glycogen reserves, and surfactant production.
Correct Answer is B
Explanation
Choice A Reason: Physiologic anemia due to maternal increased plasma volume. This is an incorrect answer that refers to a different condition that affects hemoglobin levels, not blood pressure. Physiologic anemia is a condition where the maternal plasma volume increases more than the red blood cell mass during pregnancy, which dilutes the hemoglobin concentration and lowers the hematocrit value. Physiologic anemia does not cause significant symptoms or complications in pregnant women, as it is an adaptive mechanism that enhances oxygen delivery and prevents fluid overload.
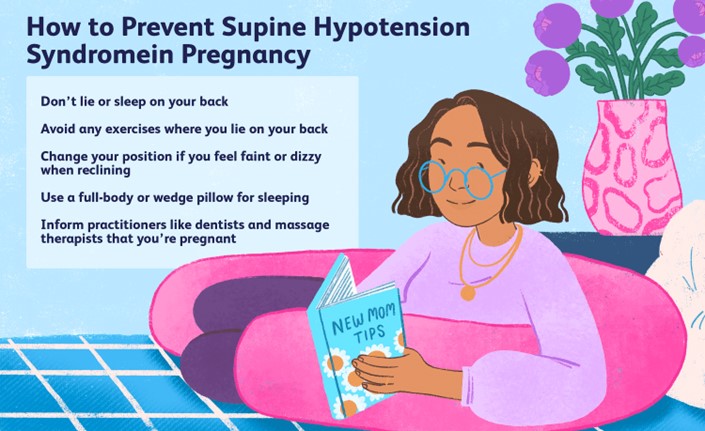
Choice B Reason: Pressure of the gravid uterus on the maternal inferior vena cava and aorta. This is because this statement explains the cause of supine hypotensive syndrome, which is a condition where lying flat on the back causes compression of the major blood vessels by the gravid uterus, which reduces venous return and cardiac output, which lowers blood pressure and perfusion to vital organs. Supine hypotensive syndrome can cause symptoms such as dizziness, lightheadedness, nausea, pallor, or syncope in pregnant women, especially in the third trimester.
Choice C Reason: Pressure of the presenting fetal part on the maternal diaphragm. This is an incorrect answer that indicates a different condition that affects respiratory function, not blood pressure. Pressure of the presenting fetal part on the maternal diaphragm is a result of cephalic engagement or lightening, which occurs when the fetal head descends into the pelvis and occupies more space in the abdominal cavity. Pressure of the presenting fetal part on the maternal diaphragm can cause symptoms such as dyspnea, heartburn, or rib pain in pregnant women.
Choice D Reason: A 50% increase in maternal blood volume during pregnancy. This is an incorrect answer that describes a normal physiological change that occurs during pregnancy, not a cause of supine hypotensive syndrome. A 50% increase in maternal blood volume during pregnancy is due to increased production of plasma and red blood cells, which helps meet the increased oxygen and nutrient demands of the fetus and placenta, and prepares the mother for blood loss during delivery. A 50% increase in maternal blood volume during pregnancy does not cause hypotension or dizziness in pregnant women.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today