A woman is at 32 weeks' gestation. Her fundal height measurement at this clinic appointment is 26 centimeters. After reviewing her ultrasound results, the health care provider asks the nurse to schedule the client for a series of ultrasounds to be done every 2 weeks. The nurse should ensure that the client understands that the main purpose for this is to:
Select one:
Rule out a suspected hydatidiform mole.
Assess for congenital anomalies.
Determine fetal presentation.
Monitor fetal growth.
The Correct Answer is D
Choice A Reason: Rule out a suspected hydatidiform mole. This is an incorrect answer that describes an unlikely condition for this client. A hydatidiform mole is a type of gestational trophoblastic disease where abnormal placental tissue develops instead of a normal fetus. A hydatidiform mole can cause vaginal bleeding, hyperemesis gravidarum (severe nausea and vomiting), preeclampsia, and hyperthyroidism. A hydatidiform mole usually causes a fundal height measurement that is larger than expected for gestational age, not smaller.
Choice B Reason: Assess for congenital anomalies. This is an incorrect answer that implies that the client has not had a previous ultrasound to screen for fetal anomalies. Congenital anomalies are structural or functional defects that are present at birth, such as cleft lip, spina bifida, or Down syndrome. Ultrasound can detect some congenital anomalies by visualizing the fetal anatomy and morphology. However, ultrasound screening for fetal anomalies is usually done between 18 and 22 weeks of gestation, not at 32 weeks.
Choice C Reason: Determine fetal presentation. This is an incorrect answer that suggests that the client has an uncertain fetal presentation. Fetal presentation is the part of the fetus that is closest to the cervix, such as vertex (head), breech (butocks or feet), or transverse (shoulder). Fetal presentation can affect the mode and outcome of delivery. Ultrasound can determine fetal presentation by locating the fetal head and spine. However, fetal presentation can also be assessed by abdominal palpation or vaginal examination, which are simpler and less invasive methods.
Choice D Reason: Monitor fetal growth. This is because fundal height measurement is a method of estimating fetal size and gestational age by measuring the distance from the pubic symphysis to the top of the uterus (fundus) in centimeters. A fundal height measurement that is significantly smaller or larger than expected for gestational age may indicate intrauterine growth restriction (IUGR) or macrosomia, respectively. IUGR means that the fetal growth is slower than expected for gestational age, which can increase the risk of fetal distress, hypoxia, acidosis, and stillbirth. Macrosomia means that the fetal weight is higher than expected for gestational age, which can increase the risk of birth injuries, shoulder dystocia, cesarean delivery, and hypoglycemia. Ultrasound is a more accurate way of assessing fetal size and growth by measuring various parameters such as biparietal diameter (BPD), head circumference (HC), abdominal circumference (AC), and femur length (FL). Ultrasound can also detect other factors that may affect fetal growth such as placental function, amniotic fluid volume, umbilical cord blood flow, and fetal anomalies.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: Applying Vaseline or lotion to newborn to maximize light absorption. This is an incorrect answer that indicates a contraindicated and harmful intervention that can interfere with phototherapy. Applying Vaseline or lotion to newborn can create a barrier or a reflective surface that can reduce the exposure and penetration of light to the skin, which can decrease the efficacy of phototherapy. Applying Vaseline or lotion to newborn can also cause skin irritation, infection, or burns, as it can trap heat and moisture under the light source.
Choice B Reason: Reducing the amount of fluid intake to 8 ounces daily. This is an incorrect answer that suggests a detrimental and dangerous intervention that can impair phototherapy. Reducing the amount of fluid intake to 8 ounces daily can cause dehydration, hypoglycemia, or electrolyte imbalance in newborns, which can worsen jaundice and increase the risk of complications such as kernicterus (brain damage due to high bilirubin levels). Reducing the amount of fluid intake to 8 ounces daily can also decrease the excretion of bilirubin through urine or stool, which can counteract the effect of phototherapy.
Choice C Reason: Keeping the newborn in the supine position. This is an incorrect answer that implies an incomplete and inadequate intervention that can limit phototherapy. Keeping the newborn in the supine position is a nursing action that involves placing the newborn on their back, which can expose their anterior body surface to light.
However, keeping the newborn in the supine position alone is not sufficient for phototherapy, as it does not expose their posterior body surface to light. The nurse should also reposition the newborn frequently to expose different body parts to light, such as their sides or abdomen.
Choice D Reason: Feeding every 3 hours to maximize intake of fluids and output. This is because feeding every 3 hours is a nursing intervention that can enhance the effectiveness and safety of phototherapy, which is a treatment that uses blue or white light to reduce the level of bilirubin in the blood. Bilirubin is a yellow pigment that is produced when red blood cells are broken down, which can cause jaundice (yellowish discoloration of the skin and mucous membranes) if it accumulates in excess. Phototherapy works by converting bilirubin into a water-soluble form that can be excreted through urine or stool. Feeding every 3 hours can increase the intake of fluids and calories, which can promote hydration, nutrition, and elimination of bilirubin.
Correct Answer is D
Explanation
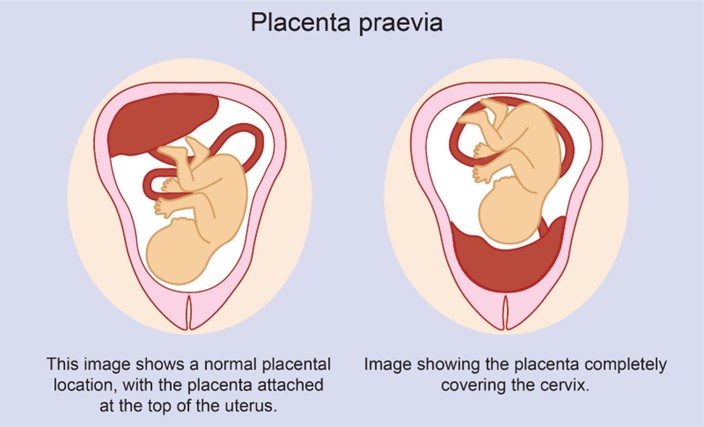
Choice A Reason: Partial placenta previa is a condition where the placenta partially covers the cervix. It usually does not resolve and may cause bleeding and complications during labor and delivery.
Choice B Reason: Complete placenta previa is a condition where the placenta completely covers the cervix. It is a serious condition that requires cesarean delivery and may cause life-threatening hemorrhage.
Choice C Reason: Marginal placenta previa is a condition where the edge of the placenta reaches the margin of the cervix. It may also cause bleeding and complications during labor and delivery.
Choice D Reason: Low-lying placenta previa is a condition where the placenta is near the cervix, but not covering it. It may resolve spontaneously as the uterus grows and the placenta moves upward.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today