In caring for the premature infant, the nurse must continually assess hydration status. Parameters to assess would include all of the following except:
Select one:
Daily weight.
Consistency of stool.
Volume of urine output.
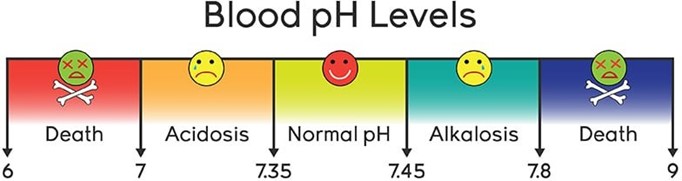
Blood pH.
The Correct Answer is D
Choice A Reason: Daily weight. This is an incorrect answer that indicates a valid parameter to assess hydration status. Daily weight is a measure of the body mass that can reflect changes in fluid balance. Daily weight can help detect fluid loss or gain in premature infants, who are more prone to dehydration or overhydration due to immature renal function and high insensible water loss.
Choice B Reason: Consistency of stool. This is an incorrect answer that indicates a valid parameter to assess hydration status. Consistency of stool is a measure of the texture and form of feces that can reflect changes in fluid intake and absorption. Consistency of stool can help identify diarrhea or constipation in premature infants, who are more susceptible to gastrointestinal problems such as necrotizing enterocolitis or feeding intolerance.
Choice C Reason: Volume of urine output. This is an incorrect answer that indicates a valid parameter to assess hydration status. Volume of urine output is a measure of the amount of urine produced and excreted by the kidneys that can reflect changes in fluid balance and renal function. Volume of urine output can help monitor hydration status and kidney function in premature infants, who are more vulnerable to fluid overload or deficit and renal impairment.
Choice D Reason: Blood pH. This is because blood pH is a measure of the acidity or alkalinity of the blood, which reflects the balance between carbon dioxide and bicarbonate in the body. Blood pH is not a direct indicator of hydration status, which refers to the amount of water and electrolytes in the body. Hydration status can affect blood pH, but blood pH can also be influenced by other factors such as respiratory or metabolic disorders.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: Macrosomic newborn. This is a correct answer that describes a possible complication of post-term pregnancy. A macrosomic newborn is a newborn that weighs more than 4000 grams or 8 pounds 13 ounces at birth. It can occur in post-term pregnancies due to prolonged exposure to maternal glucose and insulin. It can increase the risk of birth injuries, shoulder dystocia, cesarean delivery, and hypoglycemia.
Choice B Reason: Intrauterine growth restriction (IUGR). This is a correct answer that indicates a potential problem of post-term pregnancy. IUGR is a condition where the fetal growth is slower than expected for gestational age. It can occur in post-term pregnancies due to placental insufficiency, aging, or calcification, which can impair nutrient and oxygen delivery to the fetus. It can increase the risk of fetal distress, hypoxia, acidosis, and stillbirth.
Choice C Reason: Umbilical cord prolapse. This is an incorrect answer that does not reflect a risk of post-term pregnancy, but rather a risk of other factors such as prematurity, low birth weight, breech presentation, multiple gestation, polyhydramnios, or artificial rupture of membranes.
Choice D Reason: Meconium Aspiration Syndrome (MAS). This is a correct answer that denotes a possible complication of post-term pregnancy. MAS occurs when fetal stool (meconium) enters into the lungs before or during birth, causing airway obstruction, inflammation, and infection. MAS usually affects term or post-term infants who experience fetal distress or hypoxia in utero. It can cause respiratory distress syndrome (RDS), persistent pulmonary hypertension (PPHN), or chronic lung disease (CLD).
Correct Answer is A
Explanation
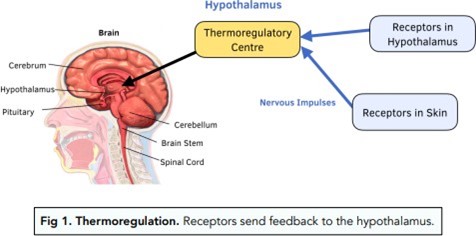
Choice A Reason: Place the infant skin to skin with the mother and re-check temperature in 30 minutes. This is because skin-to-skin contact is an effective and safe method of increasing the infant's temperature and promoting thermoregulation. Skin-to-skin contact also has other benefits such as enhancing bonding, breastfeeding, and maternal-infant attachment.
Choice B Reason: Check the infant's CBC and blood cultures, as this is a sign of probable sepsis. This is an unnecessary action that may cause undue stress and discomfort to the infant and the mother. A slightly decreased temperature in a full-term infant is not a sign of probable sepsis, but rather a common finding that may be due to environmental factors, such as exposure to cold air or wet linens.
Choice C Reason: Return the infant to the nursery for close observation under warming lights. This is an undesirable action that may interfere with the early initiation of breastfeeding and bonding between the mother and the infant. Warming lights are not recommended for routine use in healthy newborns, as they may cause dehydration, hyperthermia, or eye damage.
Choice D Reason: Notify the physician immediately and suggest orders for placement in an incubator. This is an excessive action that may indicate a lack of knowledge or confidence on the part of the nurse. An incubator is not indicated for a stable, full term infant with a slightly decreased temperature, as it may expose the infant to unnecessary interventions, infections, or separation from the mother.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today