Following a normal spontaneous vaginal delivery (NSVD), a 28 year old G3 now P3 mother develops sudden onset shortness of breath, hypoxia and cyanosis. The delivery room nurse quickly recognizes these symptoms as possible:
Select one:
Manifestations of uteroplacental insufficiency.
Manifestations of prolapsed cord.
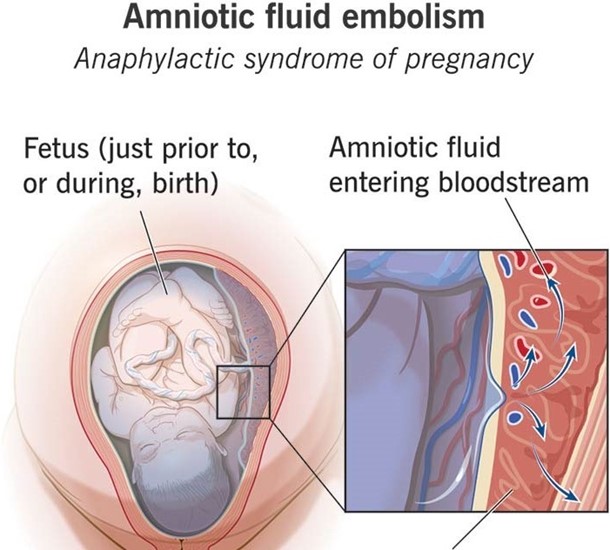
Manifestations of anaphylactoid syndrome of pregnancy.
Manifestations of an acute asthmatic episode.
The Correct Answer is C
Choice A Reason: Manifestations of uteroplacental insufficiency. This is an incorrect answer that describes a different condition that affects the fetus, not the mother. Uteroplacental insufficiency is a condition where the placenta fails to deliver adequate oxygen and nutrients to the fetus, which can result in fetal growth restriction, distress, or demise. Uteroplacental insufficiency does not cause shortness of breath, hypoxia, or cyanosis in the mother.
Choice B Reason: Manifestations of prolapsed cord. This is an incorrect answer that refers to another condition that affects the fetus, not the mother. Prolapsed cord is a condition where the umbilical cord slips through the cervix before the baby and becomes compressed by the fetal head, which can reduce oxygen flow to the fetus. Prolapsed cord does not cause shortness of breath, hypoxia, or cyanosis in the mother.
Choice C Reason: Manifestations of anaphylactoid syndrome of pregnancy. This is because anaphylactoid syndrome of pregnancy, also known as amniotic fluid embolism, is a rare and fatal condition where amniotic fluid enters into the maternal bloodstream and causes an allergic reaction, which can lead to respiratory failure, cardiac arrest, coagulopathy, and coma. Anaphylactoid syndrome of pregnancy can occur during or after labor and delivery, especially in cases of NSVD, multiparity, advanced maternal age, or placental abruption.
Choice D Reason: Manifestations of an acute asthmatic episode. This is an incorrect answer that assumes that the mother has a history of asthma or an allergic trigger. Asthma is a chronic inflammatory disorder of the airways that causes wheezing, coughing, chest tightness, and dyspnea. Asthma can be exacerbated by pregnancy or labor, but it is not a common cause of sudden onset respiratory distress in the postpartum period.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: Daily weight. This is an incorrect answer that indicates a valid parameter to assess hydration status. Daily weight is a measure of the body mass that can reflect changes in fluid balance. Daily weight can help detect fluid loss or gain in premature infants, who are more prone to dehydration or overhydration due to immature renal function and high insensible water loss.
Choice B Reason: Consistency of stool. This is an incorrect answer that indicates a valid parameter to assess hydration status. Consistency of stool is a measure of the texture and form of feces that can reflect changes in fluid intake and absorption. Consistency of stool can help identify diarrhea or constipation in premature infants, who are more susceptible to gastrointestinal problems such as necrotizing enterocolitis or feeding intolerance.
Choice C Reason: Volume of urine output. This is an incorrect answer that indicates a valid parameter to assess hydration status. Volume of urine output is a measure of the amount of urine produced and excreted by the kidneys that can reflect changes in fluid balance and renal function. Volume of urine output can help monitor hydration status and kidney function in premature infants, who are more vulnerable to fluid overload or deficit and renal impairment.
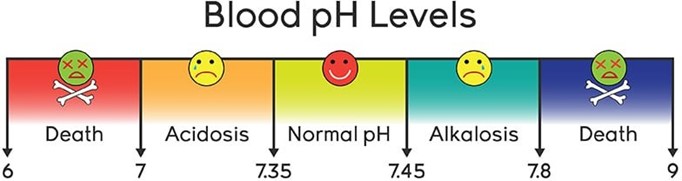
Choice D Reason: Blood pH. This is because blood pH is a measure of the acidity or alkalinity of the blood, which reflects the balance between carbon dioxide and bicarbonate in the body. Blood pH is not a direct indicator of hydration status, which refers to the amount of water and electrolytes in the body. Hydration status can affect blood pH, but blood pH can also be influenced by other factors such as respiratory or metabolic disorders.
Correct Answer is C
Explanation
Choice A Reason: Contact the physician, as it indicates early DIC. This is an incorrect answer that confuses a low pulse rate with a high pulse rate. DIC stands for disseminated intravascular coagulation, which is a life-threatening condition where abnormal clotting and bleeding occur simultaneously in the body. DIC can occur as a complication of postpartum hemorrhage, infection, or placental abruption. DIC can cause tachycardia (high pulse rate), not bradycardia (low pulse rate).
Choice B Reason: Contact the physician, as it is a first sign of postpartum eclampsia. This is an incorrect answer that misinterprets a low pulse rate as a sign of hypertension. Postpartum eclampsia is a condition where seizures occur in a woman who has preeclampsia or eclampsia after delivery. Preeclampsia and eclampsia are characterized by high blood pressure and proteinuria in pregnancy. Postpartum eclampsia can cause hypertension (high blood pressure), not hypotension (low blood pressure).
Choice C Reason: Document the finding as it is a normal finding at this time. This is because a pulse rate of 60 beats per minute is within the normal range for an adult and may reflect a physiological adaptation to the postpartum period. During pregnancy, the maternal blood volume and cardiac output increase, which can elevate the pulse rate. After delivery, these parameters gradually return to pre-pregnancy levels, which can lower the pulse rate.
Choice D Reason: Obtain an order for a CBC, as it suggests postpartum anemia. This is an incorrect answer that assumes that a low pulse rate is caused by anemia. Anemia is a condition where the red blood cell count or hemoglobin level is lower than normal, which can impair oxygen delivery to the tissues. Anemia can occur in the postpartum period due to blood loss during delivery or poor nutritional intake during pregnancy. Anemia can cause tachycardia (high pulse rate), not bradycardia (low pulse rate).

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today