The Mother-Baby nurse is caring for a two hour old newborn who is 36 4/7 weeks gestation. The nurse assesses that the newborn is experiencing tremors (jiteriness). What nursing action has the highest priority?
Select one:
Obtain a bilirubin level.
Place a pulse oximeter on the newborn.
Obtain a blood glucose level.
Take the newborn's vital signs.
The Correct Answer is C
Choice A Reason: Obtain a bilirubin level. This is an incorrect answer that indicates an irrelevant and unnecessary nursing action for a newborn with tremors or jiteriness. Obtaining a bilirubin level is a nursing action that is indicated for a newborn with jaundice (yellowish discoloration of the skin and mucous membranes), which can occur due to increased bilirubin production or decreased bilirubin excretion. Jaundice does not cause tremors or jiteriness in newborns.
Choice B Reason: Place a pulse oximeter on the newborn. This is an incorrect answer that suggests an inappropriate and insufficient nursing action for a newborn with tremors or jiteriness. Placing a pulse oximeter on the newborn is a nursing action that measures oxygen saturation and heart rate, which can indicate hypoxia (low oxygen level) or distress in newborns. Hypoxia can cause tremors or jiteriness in newborns, but it is not the only or most likely cause. Placing a pulse oximeter on the newborn does not provide enough information to diagnose or treat hypoglycemia.
Choice C Reason: Obtain a blood glucose level. This is because tremors or jiteriness are common signs of hypoglycemia (low blood glucose) in newborns, which can occur due to various factors such as prematurity, maternal diabetes, infection, or cold stress. Hypoglycemia can cause neurological damage or death if not treated promptly and effectively. Obtaining a blood glucose level is a nursing action that has the highest priority for a newborn with tremors or jiteriness, as it can confirm the diagnosis and guide the treatment.
Choice D Reason: Take the newborn's vital signs. This is an incorrect answer that implies an inadequate and delayed nursing action for a newborn with tremors or jiteriness. Taking the newborn's vital signs is a nursing action that monitors temperature, pulse, respiration, and blood pressure, which can indicate general health status and stability in newborns. Taking the newborn's vital signs may reveal signs of hypoglycemia, such as hypothermia, tachycardia, tachypnea, or hypotension, but it is not a specific or definitive test for hypoglycemia. Taking the newborn's vital signs may also waste valuable time that could be used to obtain a blood glucose level and initiate treatment.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A Reason: Place the infant skin to skin with the mother and re-check temperature in 30 minutes. This is because skin-to-skin contact is an effective and safe method of increasing the infant's temperature and promoting thermoregulation. Skin-to-skin contact also has other benefits such as enhancing bonding, breastfeeding, and maternal-infant attachment.
Choice B Reason: Check the infant's CBC and blood cultures, as this is a sign of probable sepsis. This is an unnecessary action that may cause undue stress and discomfort to the infant and the mother. A slightly decreased temperature in a full-term infant is not a sign of probable sepsis, but rather a common finding that may be due to environmental factors, such as exposure to cold air or wet linens.
Choice C Reason: Return the infant to the nursery for close observation under warming lights. This is an undesirable action that may interfere with the early initiation of breastfeeding and bonding between the mother and the infant. Warming lights are not recommended for routine use in healthy newborns, as they may cause dehydration, hyperthermia, or eye damage.
Choice D Reason: Notify the physician immediately and suggest orders for placement in an incubator. This is an excessive action that may indicate a lack of knowledge or confidence on the part of the nurse. An incubator is not indicated for a stable, full term infant with a slightly decreased temperature, as it may expose the infant to unnecessary interventions, infections, or separation from the mother.
Correct Answer is D
Explanation
Choice A Reason: Frequent voiding encourages sphincter control. This is an incorrect statement that has no relevance to labor and delivery. Sphincter control refers to the ability to contract and relax the muscles that control urination and defecation. It is not affected by frequent voiding.
Choice B Reason: A full bladder impedes oxygen flow to the fetus. This is an incorrect statement that confuses a full bladder with a prolapsed cord. A prolapsed cord is a condition where the umbilical cord slips through the cervix before the baby and becomes compressed by the fetal head, which can reduce oxygen flow to the fetus. A full bladder does not affect oxygen flow to the fetus.
Choice C Reason: Frequent voiding prevents bruising of the bladder. This is an incorrect statement that exaggerates the effect of a full bladder on the bladder wall. A full bladder may cause some pressure or discomfort on the bladder, but it does not cause bruising or damage.
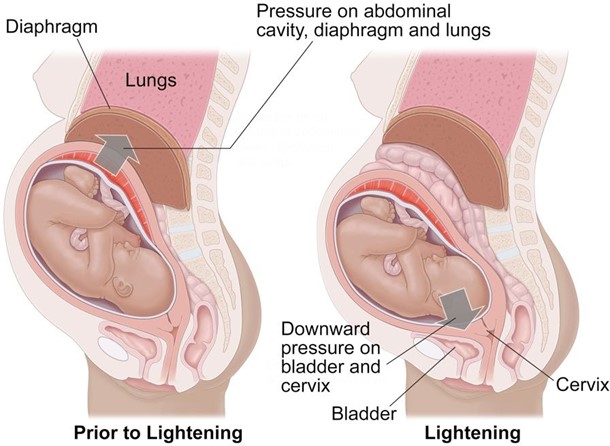
Choice D Reason: A full bladder can impede fetal descent. This is a correct statement that explains why it is important for the nurse to assess the bladder regularly and encourage the laboring client to void every 2 hours.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today