The parents of a newborn who is being treated for bacterial septicemia ask the nurse why their baby didn't seem very ill. The best response of the nurse is:
Select one:
"You would have seen more symptoms if you had been looking more closely at your baby."
"A newborn's immune system isn't mature, so symptoms are subtle and can be hard to recognize."
"A high fever will always be present in sick newborns, including your baby."
"A mother's immunity usually protects the infant from illness, but not in this case."
The Correct Answer is B
Choice A Reason: "You would have seen more symptoms if you had been looking more closely at your baby." This is an inappropriate response that blames the parents for missing the signs of sepsis and does not explain the Reason for the subtle symptoms.
Choice B Reason: "A newborn's immune system isn't mature, so symptoms are subtle and can be hard to recognize." This is an appropriate response that educates the parents about the immunological basis of sepsis in newborns and reassures them that they are not at fault for not noticing the symptoms.
Choice C Reason: "A high fever will always be present in sick newborns, including your baby." This is an incorrect response that contradicts the fact that newborns may not develop fever in response to infection due to their immature immune systems.
Choice D Reason: "A mother's immunity usually protects the infant from illness, but not in this case." This is an inaccurate response that implies that the mother failed to provide adequate immunity to her baby and does not address the question of why the baby did not seem very ill.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
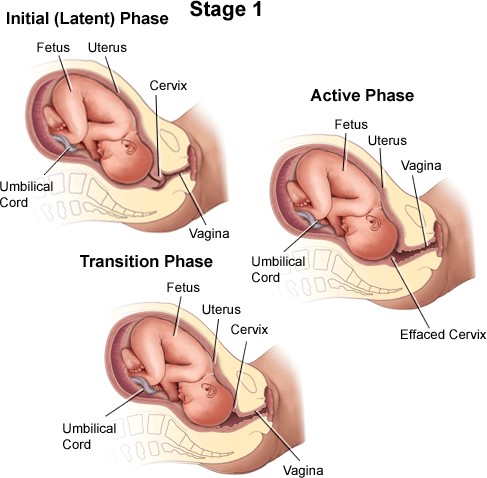
Choice A Reason: Latent phase of the first stage of labor. This is because this phase is characterized by mild and irregular contractions, slow cervical dilation (up to 4 cm), minimal cervical effacement (up to 40%), and minimal discomfort or pain. The latent phase is also known as the early phase or preparatory phase of labor.
Choice B Reason: Transition phase of the first stage of labor. This is an incorrect answer that describes a different phase with different characteristics. The transition phase is marked by strong and frequent contractions, rapid cervical dilation (from 8 to 10 cm), complete cervical effacement (100%), and intense discomfort or pain. The transition phase is also known as the terminal phase or acceleration phase of labor.
Choice C Reason: Perineal phase of the second stage of labor. This is an incorrect answer that refers to another stage and phase with different features. The second stage of labor begins with complete cervical dilation (10 cm) and ends with delivery of the baby. The perineal phase is the last part of the second stage, where the baby's head crowns and emerges through the vaginal opening.
Choice D Reason: Active phase of the first stage of labor. This is an incorrect answer that indicates another phase with different atributes. The active phase is characterized by moderate and regular contractions, progressive cervical dilation (from 4 to 8 cm), increased cervical effacement (from 40% to 80%), and increased discomfort or pain. The active phase is also known as the middle phase or dilatation phase of labor.
Correct Answer is D
Explanation
Choice A Reason: Retained placental fragments. This is an incorrect answer that refers to a different cause of late postpartum hemorrhage, which is less common than uterine atony. Retained placental fragments are pieces of placenta that remain atached to the uterine wall after delivery, which prevent uterine contraction and involution, and provide a source of bleeding and infection. Retained placental fragments can be caused by abnormal placentation (such as placenta accreta), manual removal of placenta, or incomplete separation of placenta.
Choice B Reason: Cervical or vaginal lacerations. This is an incorrect answer that refers to a different cause of late postpartum hemorrhage, which is more likely to cause early postpartum hemorrhage than late postpartum hemorrhage. Cervical or vaginal lacerations are tears or cuts in the cervix or vagina that occur during delivery, which can cause bleeding from the damaged blood vessels. Cervical or vaginal lacerations can be caused by rapid or instrumental delivery, large or malpositioned fetus, or episiotomy.
Choice C Reason: Uterine inversion. This is an incorrect answer that refers to a different cause of late postpartum hemorrhage, which is rare and life-threatening. Uterine inversion is a condition where the uterus turns inside out and protrudes through the cervix and vagina after delivery, which can cause massive bleeding and shock. Uterine inversion can be caused by excessive traction on the umbilical cord, fundal pressure, or uterine relaxation.
Choice D Reason: Uterine atony. This is because uterine atony is a condition where the uterus fails to contract and retract after delivery, which leads to bleeding from the placental site. Uterine atony is the most common cause of late postpartum hemorrhage, accounting for about 75% of cases. Late postpartum hemorrhage is excessive bleeding from the uterus or genital tract that occurs more than 24 hours but less than 12 weeks after delivery. Late postpartum hemorrhage can be caused by retained placental fragments, subinvolution of the uterus, infection, or coagulation disorders.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today