Which intervention is most important for the practical nurse (PN) to implement for a client who is receiving total parenteral nutrition (TPN)?
Collect fingerstick glucose levels
Implement bleeding precautions
Obtain daily weights
Check urine for albumin
The Correct Answer is A
a) Collect fingerstick glucose levels. Correct
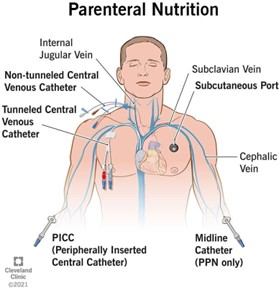
Collecting fingerstick glucose levels is the most important intervention for the PN to implement for a client who is receiving TPN. TPN is a method of feeding that bypasses the gastrointestinal tract and provides all the nutritional needs of the body through a vein. TPN contains a high concentration of glucose, which can cause hyperglycemia or fluctuations in blood sugar levels. Therefore, it is essential to monitor the client's glucose levels frequently and adjust the infusion rate or insulin administration accordingly.
b) Implement bleeding precautions.
Implementing bleeding precautions is not the most important intervention for the PN to implement for a client who is receiving TPN. Bleeding precautions are measures to prevent or minimize bleeding in clients who have a high risk of hemorrhage due to conditions such as thrombocytopenia, coagulopathy, or anticoagulant therapy. TPN does not directly increase the risk of bleeding, although it may affect the liver function and clotting factors in some cases². Therefore, bleeding precautions are not a priority for a client who is receiving TPN.
c) Obtain daily weights.
Obtaining daily weights is not the most important intervention for the PN to implement for a client who is receiving TPN. Obtaining daily weights is a way to monitor the client's fluid balance, nutritional status, and response to therapy. TPN can cause fluid overload, dehydration, or electrolyte imbalances in some cases²⁵. Therefore, obtaining daily weights is important, but not as important as monitoring glucose levels.
d) Check urine for albumin.
Checking urine for albumin is not the most important intervention for the PN to implement for a client who is receiving TPN. Checking urine for albumin is a way to detect proteinuria, which is an indicator of kidney damage or disease. TPN does not directly cause kidney problems, although it may affect the renal function and urine output in some cases². Therefore, checking urine for albumin is not a priority for a client who is receiving TPN.
 |
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: Proactive prevention is not a level of prevention, but a type of prevention that involves anticipating and avoiding potential health problems before they occur.
Choice B reason: Secondary prevention is a level of prevention that involves screening, early detection, and prompt treatment of health problems to prevent complications and limit disability.
Choice C reason: Tertiary prevention is a level of prevention that involves rehabilitation, restoration, and support of health and function after a health problem has caused damage or disability.
Choice D reason: Primary prevention is a level of prevention that involves health promotion and protection of health and well-being by reducing or eliminating risk factors and preventing the onset of disease or injury.
Correct Answer is D
Explanation
- Child abuse is the intentional or neglectful physical, emotional, or sexual harm or injury of a child by a parent, caregiver, or another person who has a relationship of trust or responsibility with the child. Child abuse can have serious and long-lasting consequences for the child's health, development, and well-being.
- The practical nurse (PN) has a legal and ethical duty to identify, report, and prevent child abuse. The PN should be alert for any signs and symptoms of child abuse, such as unexplained or inconsistent injuries, bruises, burns, fractures, or scars; behavioural changes, such as fear, anxiety, aggression, withdrawal, or depression; poor hygiene, nutrition, or growth; lack of supervision, medical care, or education; or sexualized behaviours or knowledge.
- The PN should also conduct a thorough and sensitive assessment of the child and the family situation, using open-ended questions, active listening, and a non-judgmental attitude. The PN should compare the history and physical findings of the child with the expected developmental milestones and normal variations for the child's age and stage. The PN should also document any relevant information in an objective and factual manner.
- When the mother of a school-aged boy tells the PN that he fell out of a tree and hurt his arm and shoulder, the PN should assess the child's injury and compare it with the mother's explanation. The most significant indicator of possible child abuse in this scenario is if the injury description by the mother varies from the child's version. This may suggest that the mother is lying or covering up the true cause of the injury, which may be intentional or accidental harm by herself or someone else. A discrepancy between the mother's and the child's stories may also indicate that the child is afraid or coerced to hide the truth about the abuse.
- Therefore, option D is the correct answer, while options A, B, and C are incorrect.
- Option A is incorrect because the child looking at the floor when answering the nurse's questions may not be a sign of abuse, but rather a sign of shyness, embarrassment, pain, or discomfort.
Option B is incorrect because the mother describing in detail what she did for her injured child may not be a sign of abuse, but rather a sign of concern, care, or guilt.
Option C is incorrect because the abrasions on the child's arms, legs, and chest having healed may not be a sign of abuse, but rather a sign of normal wound healing or previous accidents.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today