When measuring the size, depth, and wound tunneling of a client's stage 4 pressure injury, what action should the nurse perform first?
Perform hand hygiene.
Assess the condition of the visible wound bed.
Measure the width of the wound with a disposable ruler.
Insert a swab into the wound at 90 degrees.
The Correct Answer is A
Choice A rationale: Performing hand hygiene before any wound care procedure is essential to prevent infection and maintain aseptic technique.
Choice B rationale: Assessing the condition of the visible wound bed is an important step but not the first action. Hand hygiene should precede any assessment or intervention.
Choice C rationale: Measuring the width of the wound with a disposable ruler is part of the wound measurement process but should follow hand hygiene.
Choice D rationale: Inserting a swab into the wound at 90 degrees is not the first step. Hand hygiene and assessment should precede any invasive procedures.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A rationale: Protective supine positioning is not ideal for managing dysphagia or facilitating swallowing.
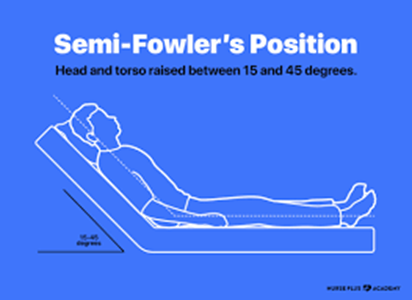
Choice B rationale: Semi-Fowlers positioning, with the head of the bed elevated at a 30 to 45-degree angle, is often recommended for clients with dysphagia. This position helps prevent aspiration during eating and promotes effective swallowing.
Choice C rationale: Low-Fowlers and Fowlers positions may not be as effective in preventing aspiration during eating as the Semi-Fowlers position.
Choice D rationale: Fowlers positioning alone may not be sufficient for managing dysphagia; Semi-Fowlers is a more specific recommendation.
Correct Answer is C
Explanation
Choice A rationale: While dietary fiber is important for bowel health, raw vegetables can be harder to digest. Cooking or steaming vegetables may be a more suitable option for some individuals with constipation.
Choice B rationale: Limiting activity can contribute to constipation, as physical activity helps stimulate bowel movements.
Choice C rationale: Drinking four to five glasses of water daily is important for maintaining hydration and supporting normal bowel function. Dehydration can contribute to constipation.
Choice D rationale: Bearing down hard when defecating may increase the risk of complications and is not a recommended strategy for relieving constipation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today