A nurse is completing a chart audit and finds the following wound documented as a Stage I Pressure Ulcer. The nurse recognizes this is incorrect. How should the wound have been classified?

Deep Tissue Injury
Stage III Pressure Ulcer
Unstageable Ulcer
Stage IV Pressure Ulcer
The Correct Answer is A
Choice A rationale: A deep tissue injury involves intact skin with a purple or maroon localized area of discolored, non-blanchable, deep red or maroon, or a blood-filled blister due to damage of underlying soft tissue from pressure or shear. It is a stage that is more appropriate for the described wound involving the epidermis and dermis.
Choice B rationale: Stage III pressure ulcers involve full-thickness tissue loss, but they do not involve the epidermis and dermis.
Choice C rationale: Unstageable ulcers are covered with slough or eschar, making it difficult to determine the depth of tissue involvement. In this case, the wound's description indicates involvement of the epidermis and dermis.
Choice D rationale: Stage IV pressure ulcers involve full-thickness tissue loss with exposed bone, tendon, or muscle, not just the epidermis and dermis.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A rationale: Protective supine positioning is not ideal for managing dysphagia or facilitating swallowing.
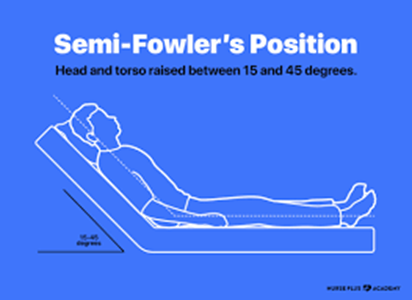
Choice B rationale: Semi-Fowlers positioning, with the head of the bed elevated at a 30 to 45-degree angle, is often recommended for clients with dysphagia. This position helps prevent aspiration during eating and promotes effective swallowing.
Choice C rationale: Low-Fowlers and Fowlers positions may not be as effective in preventing aspiration during eating as the Semi-Fowlers position.
Choice D rationale: Fowlers positioning alone may not be sufficient for managing dysphagia; Semi-Fowlers is a more specific recommendation.
Correct Answer is B
Explanation
Choice A rationale: Extension is the movement of a body part away from the midline.
Choice B rationale: Adduction is the movement of a body part toward the midline.
Choice C rationale: Circumduction is the circular movement at the joint.
Choice D rationale: Abduction is the movement of a body part away from the midline.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today