When admitting a client with a diagnosis of transient ischemic attack (TIA), which intervention is most important for the nurse to include in this client's plan of care?
Assess bilateral breath sounds.
Palpate the suprapubic region for urinary retention.
Review the client's daily medications.
Initiate neurological monitoring every 2 hours.
The Correct Answer is D
Choice A reason: While assessing breath sounds is part of a comprehensive evaluation, it is not the most critical intervention for a TIA, which primarily affects neurological function.
Choice B reason: Palpating the suprapubic region for urinary retention is important but not the priority intervention for a client with TIA, as it does not directly relate to the risk of stroke.
Choice C reason: Reviewing the client's daily medications is necessary for overall care but is not the most immediate concern upon admission for a TIA.
Choice D reason: Initiating neurological monitoring every 2 hours is essential for a client with TIA to promptly identify any changes or progression in neurological status, which could indicate a stroke. This is the most important intervention to include in the plan of care for a client admitted with TIA. Neurological monitoring allows for immediate intervention if the client's condition worsens, potentially preventing further ischemic damage.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: Avoiding sunscreen is not recommended as it increases the risk of skin cancer; vitamin D can be obtained safely through diet and supplements.
Choice B reason: While it is true that vitamin D and calcium are balanced with phosphorus, this statement does not directly encourage compliance with supplementation.
Choice C reason: Although calcium uses vitamin D produced by sunlight exposure, relying solely on sunshine is not sufficient, especially for individuals at risk of osteoporosis.
Choice D reason: Emphasizing that vitamin D enhances calcium absorption into the bone provides a clear rationale for the client to comply with the supplementation regimen.
Correct Answer is A
Explanation
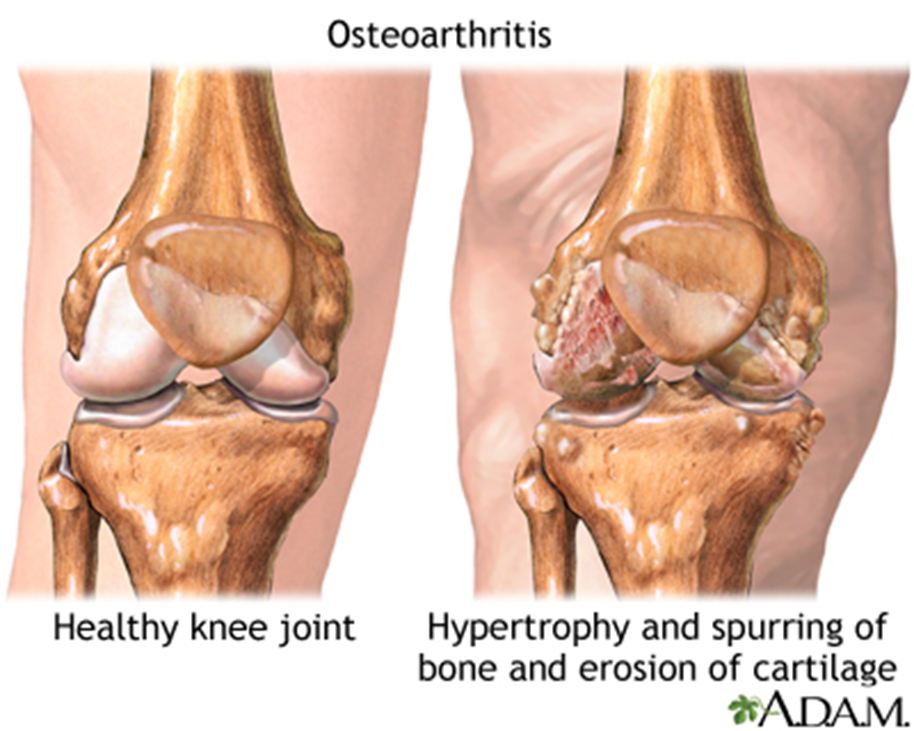
Choice A reason: Asking the client to describe the pain is essential as it provides subjective information about the pain's quality, intensity, and impact on daily activities, which is crucial for assessing osteoarthritis pain.
Choice B reason: Observing body language and movement can offer insights into the pain's impact on function, but it does not replace the client's verbal description of the pain experience.
Choice C reason: Identifying effective pain relief measures is part of managing osteoarthritis but does not directly assess the quality of the client's knee pain.
Choice D reason: Providing a numeric pain scale is a method to quantify pain intensity but may not fully capture the quality or characteristics of the pain.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today