The practical nurse (PN) observes a client’s initial postoperative dressing, which is saturated with serosanguinous fluid, and a drainage device that appears partially compressed. Which follow-up actions should the PN implement? (Select all that apply.).
Document the appearance of the wound as inflamed.
Report the appearance of the dressing to the charge nurse.
Remove the drainage device and apply a pressure dressing.
Compress the drainage device before closing the tab.
Clamp the drainage tubing for the next four hours.
Correct Answer : B,D
The correct answers are Choice B and D:
Choice B: Report the appearance of the dressing to the charge nurse,
Choice D: Compress the drainage device before closing the tab.
Choice A rationale:
Documenting the appearance of the wound as inflamed is not appropriate. As a practical nurse, the immediate concern is to take action and report any concerning findings to the appropriate healthcare provider rather than just documenting it.
Choice B rationale:
Reporting the appearance of the dressing to the charge nurse is essential. The charge nurse or a more experienced healthcare provider needs to be informed of any abnormal findings or signs of infection for further evaluation and appropriate intervention.
Choice C rationale:
Removing the drainage device and applying a pressure dressing is not within the scope of practice for a practical nurse. These actions require a higher level of expertise and are typically performed by a registered nurse or healthcare provider.
Choice D rationale:
Compressing the drainage device before closing the tab is a correct action. This helps to ensure that the device is functioning properly, and there are no leaks or obstructions in the drainage system.
Choice E rationale:
Clamping the drainage tubing for the next four hours is not recommended unless specifically ordered by a healthcare provider. Clamping the drainage tubing without appropriate orders may disrupt the normal drainage process and cause complications.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
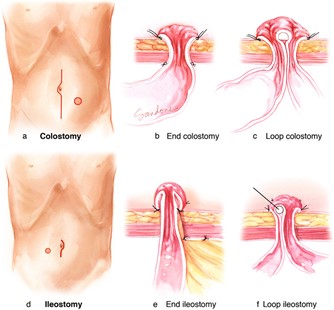
This is the best action for the PN to implement because it addresses the client's question and provides an opportunity to educate the client about fecal diversion surgery and its outcomes. The PN should review the type, location, and appearance of the surgical opening (stoma) and explain how it will affect the client's elimination and body image.
B. Verifying that the client had nothing by mouth (NPO) for the past 24 hours is not relevant to the client's question and does not provide any information or support.
C. Asking the client if he finished the bowel sterilization prescription is not relevant to the client's question and does not provide any information or support.
D. Determining if this is the first indwelling catheter the client has had is not relevant to the client's question and does not provide any information or support.
Correct Answer is B
Explanation
The correct answer is Choice B. Refer to the dermatologist for prescribed long-term therapy. Choice A rationale:
Omitting specific foods like chocolate, carbonated drinks, and fried foods from the diet is a common misconception about acne management. While a healthy diet can contribute to overall skin health, there is no direct evidence to support the notion that avoiding these foods alone will effectively treat acne. Acne is a complex skin condition influenced by various factors, including hormonal imbalances and genetics.
Choice B rationale:
Referring the client to a dermatologist for prescribed long-term therapy is the most appropriate recommendation for managing acne. Dermatologists are medical professionals specialized in skin conditions and can provide personalized treatment plans based on the client's specific type and severity of acne. They may prescribe topical or oral medications, such as retinoids, antibiotics, or hormonal therapy, to effectively manage acne.
Choice C rationale:
Expressing blackheads and using an exfoliating scrub is not a recommended approach for managing acne. Manual extraction of blackheads can lead to skin irritation, infection, and scarring. Exfoliating scrubs can also cause damage to the skin, especially if used too frequently or if the acne is inflamed.
Choice D rationale:
Washing the hair and skin daily with mild soap and warm water is a general hygiene recommendation and may help to keep the skin clean, but it is not a specific and effective treatment for acne. Acne requires targeted therapies to address its underlying causes and manage its symptoms.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today