A client who is 39 weeks gestation calls the labor and delivery unit to report that she is experiencing mild, irregular contractions. She tells the practical nurse (PN) that the healthcare provider examined her in the clinic today, and her cervix was 3 cm dilated, with intact membranes, and the presenting part was at -1 station. Which intervention should the PN implement?
Tell her to empty her bladder and call if she has a bloody show.
Direct her to come to the unit for impending delivery.
Ask the charge nurse for further instructions.
Encourage ambulation until the contractions are regular.
The Correct Answer is A
The correct answer is choice A: Tell her to empty her bladder and call if she has a bloody show.
Choice A rationale:
The client is 39 weeks gestation and experiencing mild, irregular contractions. The fact that her cervix is already 3 cm dilated and the presenting part is at -1 station indicates that she is in early labor. Emptying the bladder can help relieve pressure on the cervix and promote progress in labor. Instructing her to call if she has a bloody show is essential because it could indicate that her labor is advancing, and she may need to come to the labor and delivery unit soon.
Choice B rationale:
Directing her to come to the unit for impending delivery is not appropriate at this stage, as she is only experiencing mild, irregular contractions and is likely in early labor. Coming to the unit too early may lead to unnecessary interventions and discomfort for the client.
Choice C rationale:
Asking the charge nurse for further instructions is not necessary in this situation. The client's condition is not emergent, and the practical nurse can handle the situation appropriately based on the information provided.
Choice D rationale:
Encouraging ambulation until the contractions are regular might be beneficial in some cases to promote labor progress. However, given that the client is already 3 cm dilated and experiencing mild, irregular contractions, it's better to address the issue of bladder emptying and potential bloody show.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
The correct answer is choice D, Pupils reactive to accommodation. Choice A rationale:
"Peripheral vision intact”. refers to the ability to see objects at the outer edges of one's visual field. It is not relevant to the assessment of pupillary response and does not describe the finding of pupils constricting as they change focus from a far object to a near object.
Choice B rationale:
"Nystagmus present with pupillary focus”. suggests involuntary rapid eye movements accompanied by changes in pupillary response. Nystagmus is not an expected finding during pupillary accommodation, and its presence would indicate a neurological issue rather than a normal response.
Choice C rationale:
"Consensual pupillary constriction present”. refers to both pupils constricting when light is shined into one eye. While this finding is normal, it does not specifically describe the pupils' response during accommodation when focusing from a far object to a near object.
Choice D rationale:
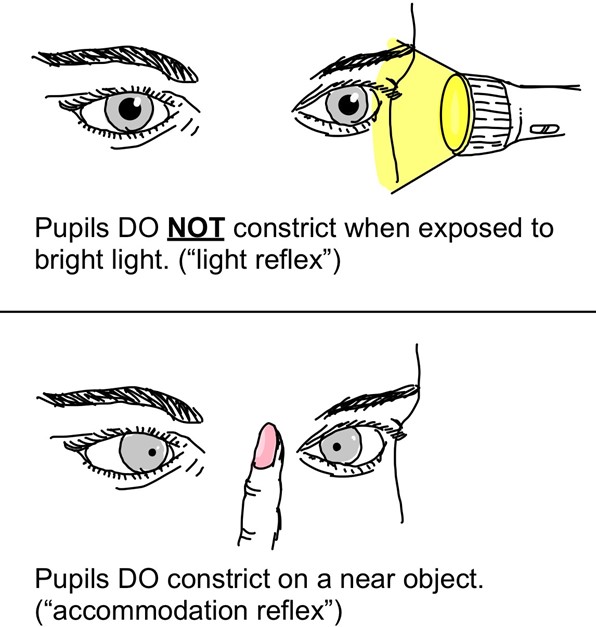
"Pupils reactive to accommodation”. accurately describes the normal physiological response of the pupils constricting as they change focus from a distant object to a nearby object. This response ensures that the appropriate amount of light enters the eyes to maintain clear vision during different distances of focus.
Correct Answer is D
Explanation
d. Escort the client to a calm and quiet place.
The PN should use a calm and firm approach to de-escalate the situation and remove the client from the stressful environment. This can help prevent further agitation and potential violence.
The other options are not correct because:
- Instructing a UAP to stay with the client may not be effective or safe, as the UAP may not have the skills or training to handle an agitated client.
- Notifying the client's healthcare provider is not a priority action, as it does not address the immediate safety of the client and others.
- Administering a PRN medication for agitation may be indicated, but it is not the first action. The PN should try non- pharmacological interventions first, unless there is an imminent risk of harm.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today