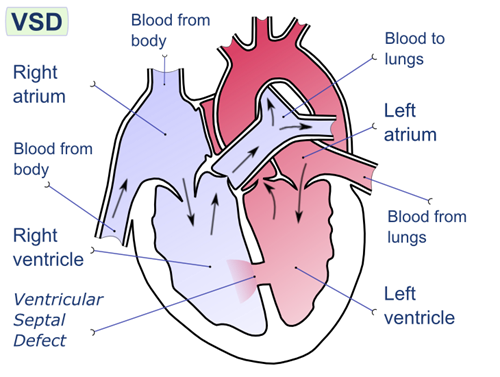
The practical nurse (PN) is feeding a 2-month-old male infant with heart failure due to a ventricular septal defect (VSD). Which intervention should the PN implement?
Weigh before and after feeding.
Allow the infant to rest before feeding.
Feed the infant when he cries.
Insert a nasogastric feeding tube.
The Correct Answer is B
In infants with heart failure, they may have difficulty feeding due to fatigue and increased work of breathing. Allowing the infant to rest before feeding helps conserve their energy and reduces the risk of excessive fatigue during feeding.
The other options are not appropriate interventions for this situation:
A. Weigh before and after feeding: Weighing before and after feeding is not necessary in this case unless specifically ordered by the healthcare provider. It is not directly related to the management of feeding an infant with heart failure.
C. Feed the infant when he cries: Feeding the infant solely based on crying may not be appropriate in this case. It is important to establish a feeding schedule and monitor the infant's signs of hunger and satiety to ensure adequate nutrition and prevent overfeeding.
D. Insert a nasogastric feeding tube: Inserting a nasogastric feeding tube should not be the first intervention unless there is a specific indication or order from the healthcare provider. In this scenario, the focus is on supporting oral feeding and allowing the infant to rest before feeding.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
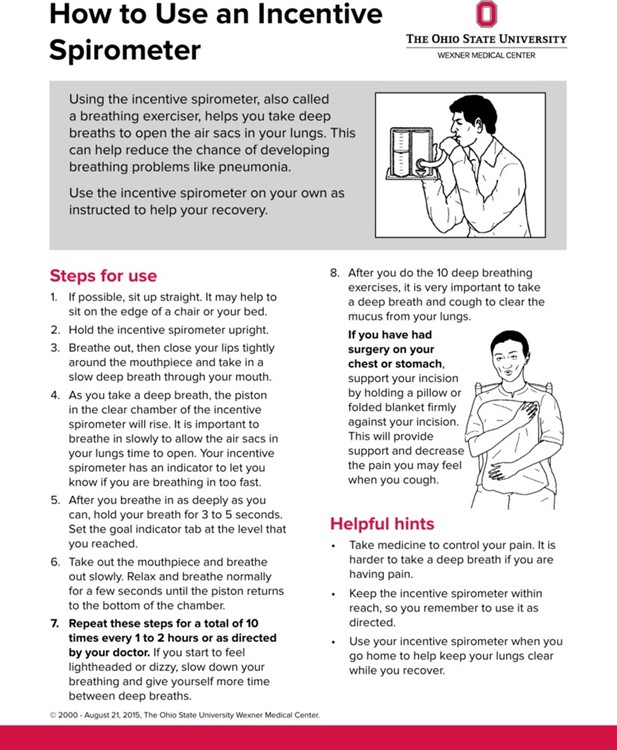
The practical nurse (PN) should reteach the proper use of the spirometer when the client demonstrates blowing forcefully into the mouthpiece. The proper way to use an incentive spirometer is to sit upright, hold the spirometer upright, place your mouth around the mouthpiece, breathe out slowly, and then inhale slowly only through your mouth as deeply as you can. Blowing forcefully into the mouthpiece is not the correct way to use an incentive spirometer.
B. Exhaling slowly after two seconds: This is actually a correct action when using an incentive spirometer. The proper way to use an incentive spirometer is to exhale slowly before inhaling deeply.
C. Using a tight seal around the mouthpiece: This is also a correct action when using an incentive spirometer. It’s important to create a tight seal around the mouthpiece with your lips to ensure that you’re inhaling and exhaling only through your mouth.
D. Sitting upright during the treatment: This is another correct action when using an incentive spirometer. Sitting upright helps you to breathe more deeply and fully, which is the goal of using an incentive spirometer.
Correct Answer is C
Explanation
When assessing an older client with left-sided heart failure (HF), the most important intervention for the practical nurse (PN) to implement is to auscultate all lung fields. Left-sided heart failure is characterized by the inability of the left ventricle to effectively pump blood, leading to fluid accumulation in the lungs. Auscultating all lung fields allows the PN to assess for the presence of abnormal lung sounds such as crackles, indicating pulmonary congestion.
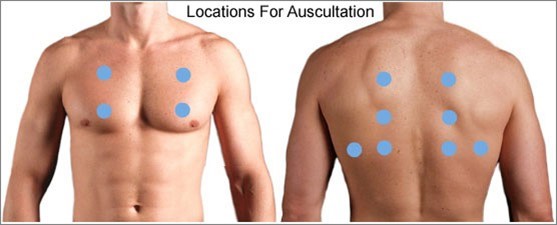
In summary, when assessing an older client with left-sided heart failure, the most important intervention for the practical nurse (PN) to implement is to auscultate all lung fields. This allows for the detection of abnormal lung sounds associated with pulmonary congestion, a hallmark sign of left-sided heart failure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today