The mother of a school-aged boy tells the practical nurse (PN) that he fell out of a tree and hurt his arm and shoulder. Which assessment should the practical nurse (PN) note as the most significant indicator of possible child abuse?
The injury description by the mother varies from the child's version.
The child looks at the floor when answering the nurse's questions.
The abrasions on the child's arms, legs, and chest have healed.
The mother describes in detail what she did for her injured child.
The Correct Answer is A
The injury description by the mother varies from the child's version.
Choice A rationale:
The practical nurse (PN) should note the significant indicator of possible child abuse, which is the discrepancy between the mother's description of the injury and the child's version. In cases of child abuse, perpetrators often provide inconsistent or conflicting explanations about how the injuries occurred, raising suspicion of maltreatment. This inconsistency can be a red flag for the PN to further assess the situation and, if necessary, report concerns to the appropriate authorities.
Choice B rationale:
While the child looking at the floor when answering questions might be a behavior worth noting, it alone is not a definitive indicator of child abuse. Children may exhibit various emotional responses for various reasons, and it requires further assessment to determine if there are signs of abuse.
Choice C rationale:
The healing of abrasions on the child's arms, legs, and chest does not necessarily indicate child abuse. Children are active and prone to minor injuries, which are a normal part of growing up. The PN should investigate further to determine the cause of the injuries.
Choice D rationale:
The mother describing in detail what she did for her injured child does not automatically suggest child abuse. It is essential for the PN to gather more information and conduct a comprehensive assessment before drawing any conclusions.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
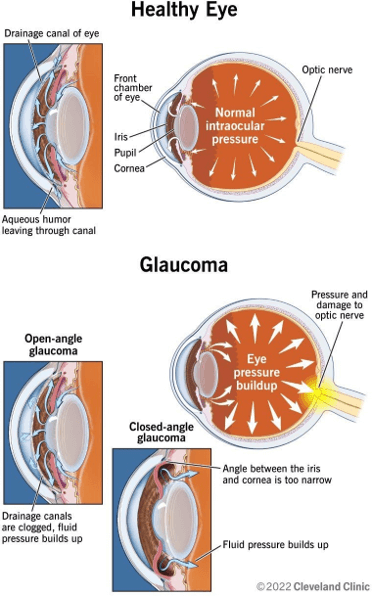
Glaucoma is a group of eye diseases that damage the optic nerve and cause vision loss. It is often associated with increased intraocular pressure, which can compress the nerve fibers and reduce blood flow to the retina. The most common type of glaucoma, open-angle glaucoma, causes gradual loss of peripheral vision.
The other options are not correct because:
- Macular edema is a condition that causes swelling and fluid accumulation in the macula, the central part of the retina that is responsible for sharp and detailed vision. It can cause blurred or distorted vision, but it does not affect the optic nerve or the peripheral vision.
- Cataract is a condition that causes clouding of the lens, which is the transparent structure that focuses light onto the retina. It can cause blurred, dim, or yellowed vision, but it does not affect the optic nerve or the intraocular pressure.
- Diabetic retinopathy is a complication of diabetes that damages the blood vessels in the retina and causes bleeding, leakage, or scarring. It can cause blurred, fluctuating, or darkened vision, but it does not affect the optic nerve or the intraocular pressure.
Correct Answer is B
Explanation
The correct answer is choice B: Children need time to actively explore their environment. Choice A rationale:
Playpens do provide a sense of security for the child, but confining the child solely to the playpen might hinder their developmental needs. While it is essential to have a safe space for a toddler, children also require opportunities to explore and engage with their environment actively.
Choice B rationale:
The practical nurse (PN) should use this rationale when responding to the parent. Children, especially toddlers, learn and develop crucial skills through active exploration of their environment. Being confined to a playpen for extended periods may limit their opportunities for learning, hinder their physical development, and restrict social interaction, which are essential aspects of their growth.
Choice C rationale:
While playpens can provide a safe environment for a toddler when used appropriately and under supervision, keeping the child confined for the sole purpose of preventing dirtiness is not recommended. Overusing playpens can hinder a child's natural curiosity and desire to explore, potentially affecting their overall development.
Choice D rationale:
While over-concern about appearance can be harmful in some contexts, it is not directly related to the child being kept in a playpen to avoid getting dirty. The primary concern here is about providing the child with adequate opportunities for exploration, growth, and development, rather than focusing solely on appearance.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today