The nurse notes that a client has ataxia. Which test does the nurse use to gain more information about this client's gait?
Plantar flexion
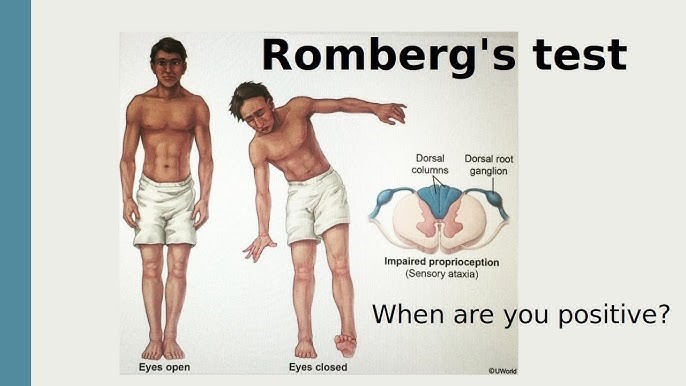
Romberg
Achilles reflex
Patellar reflex
The Correct Answer is B
Choice A reason: Plantar flexion is the movement of the foot that points the toes downward. It is not a test for gait, but rather a test for muscle strength and nerve function in the lower leg.
Choice B reason: Romberg is a test for balance and coordination that involves asking the client to stand with their feet together and arms at their sides, first with their eyes open and then with their eyes closed. If the client sways or falls when their eyes are closed, it indicates a problem with their proprioception, which is the sense of position and movement of the body. Ataxia is a condition that affects proprioception and causes impaired gait, so Romberg is an appropriate test for it.
Choice C reason: Achilles reflex is the contraction of the calf muscle when the Achilles tendon is tapped. It is not a test for gait, but rather a test for spinal cord function and nerve damage in the lower leg.
Choice D reason: Patellar reflex is the extension of the lower leg when the patellar tendon is tapped. It is not a test for gait, but rather a test for spinal cord function and nerve damage in the upper leg.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["C","D"]
Explanation
Choice A reason: The inability to take risks is not a quality of an effective nurse leader, as it may limit the leader's potential for growth, innovation, and improvement. Effective nurse leaders are willing to take calculated risks that are based on evidence, experience, and intuition. They are also able to learn from their mistakes and failures and use them as opportunities for development.
Choice B reason: Never consider being a follower is not a quality of an effective nurse leader, as it may indicate a lack of flexibility, collaboration, and respect for others. Effective nurse leaders are able to adapt to different situations and roles, depending on the needs and goals of the team. They are also able to recognize the strengths and contributions of their followers and empower them to achieve their full potential.
Choice C reason: The ability to set priorities is a quality of an effective nurse leader, as it helps the leader to focus on the most important and urgent tasks and goals. Effective nurse leaders are able to identify the needs and expectations of their clients, staff, and organization, and allocate their time, resources, and energy accordingly. They are also able to delegate tasks appropriately and efficiently.
Choice D reason: Integrity is a quality of an effective nurse leader, as it reflects the leader's honesty, trustworthiness, and ethical standards. Effective nurse leaders are able to act in accordance with their values and principles, and uphold the professional code of conduct. They are also able to communicate openly and transparently, and accept responsibility and accountability for their actions and decisions.
Choice E reason: Critical care certification is not a quality of an effective nurse leader, as it is not a requirement or a guarantee for leadership success. Critical care certification is a credential that demonstrates the nurse's knowledge and competence in providing care to critically ill patients. While it may enhance the nurse's clinical skills and confidence, it does not necessarily reflect the nurse's leadership skills or abilities. Effective nurse leaders can come from various backgrounds and specialties, as long as they have the necessary qualities and attributes that enable them to lead others effectively.
Correct Answer is A
Explanation
Choice A reason: "Move objects away from the client." This instruction should be included in the teaching. It is a safety measure that can prevent injury or harm to the client during a seizure. Moving objects away from the client can create more space and avoid contact with sharp, hard, or hot items.
Choice B reason: "Restrain the client." This instruction should not be included in the teaching. It is a harmful action that can worsen or prolong the seizure. Restraining the client can interfere with their natural movements, cause pain or discomfort, or damage their muscles or joints.
Choice C reason: "Place the client on his back." This instruction should not be included in the teaching. It is a dangerous position that can compromise the client's airway and breathing. Placing the client on his back can increase the risk of choking, aspiration, or suffocation.
Choice D reason: "Insert a padded tongue blade into the client's mouth." This instruction should not be included in the teaching. It is an outdated and ineffective practice that can cause more harm than good. Inserting a padded tongue blade into the client's mouth can damage their teeth, gums, tongue, or lips, or block their airway. Contrary to popular belief, it is impossible for a person to swallow their tongue during a seizure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today